
Atorvastatin
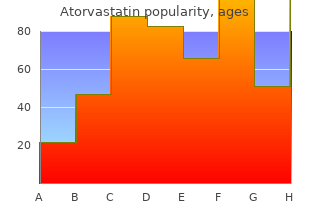
"20 mg atorvastatin, cholesterol chart mg/dl."
By: William A. Weiss, MD, PhD
- Professor, Neurology UCSF Weill Institute for Neurosciences, University of California, San Francisco, San Francisco, CA

https://profiles.ucsf.edu/william.weiss
These are; routine violations which occur when individuals believe that they have enough skill to break rules and this can be done in order to save time; situational violations order atorvastatin 10mg on line cholesterol ratio tc/hdl, occurring when the local environment makes following the rules difficult or impossible; Optimising violations purchase atorvastatin 20 mg without a prescription cholesterol score of 8, which occur for personal gain generic 10mg atorvastatin free shipping definition of cholesterol in hindi, 13 such as deciding to break a rule to demonstrate skill at a particular task buy atorvastatin 5mg with mastercard cholesterol test houston. ure 3 depicts this systems perspective and shows the path that an error takes, including not only the active failures or unsafe acts but also latent conditions . We then explored the error-producing conditions and latent conditions associated with each error, depicting the factors in a diagram. This led to the formation of an overall model of the different types of errors, according to Reasons framework. As with the prevalence study, a validation panel was set up to assess the potential severity of the reported errors using the same technique described previously (see section 3. The interview schedule the interview schedule for the telephone interviews is given in Appendix F. This schedule refined by discussion with members of the expert reference group, covered areas the type of programme provided to students, elements of the course that covered prescribing, interdisciplinary teaching, assessments and feedback. Also, importantly, it asked whether interviewees believed that their curriculum prepared students for prescribing and whether is had any gaps. The curriculum leads in each of those medical schools were identified and approached with a view to participating in this study. Analysis Thematic analysis was carried out with data collected from the curriculum leads. Fourteen doctors worked in a teaching hospital trust and 16 worked in a district general hospital at the time of the interview. They are from 17 different hospital sites, representing over half of the 29 hospital trusts in the North-West. Five interviewees were of Asian ethnicity, two of black ethnicity, and the remainder of white ethnicity. Individual codes are not assigned in this table so as to ensure anonymity for both the medical school and the interviewee. In some schools, the curriculum leads nominated an alternative interviewee who was more familiar with the detailed delivery of the pharmacology and therapeutics curriculum. Each medical school was assigned a letter from A- R and these are used in subsequent quotations. On commencing the interview, a few doctors could not remember making any prescribing errors. However, reflection during the interview and prompting about interactions with pharmacists led all interviewees to recall at least one prescribing error, some reporting up to eight. Their initial difficulty remembering errors suggests they were not especially anxious about errors nor did they find prescribing overly problematic. Interviewees strongly suspected they had made more errors than they actually knew about. This issue was often discussed during recruitment presentations, when potential recruits said they felt sure that they had made errors but didnt actually know what they were and therefore it might be hard to discuss them in a research interview. When interviewees were asked to recall prescribing errors, they often distinguished between silly errors and more serious errors. Those that were categorised as silly included prescribing statins during the day instead of at 42 night; serious errors were generally related to errors in dosage. Errors that were perceived as silly could also result from a doctors conscious decision to overlook some aspect of prescribing, leading to what could be described as a violation. This type of error usually resulted from a heavy workload under time pressure, a situation discussed in greater detail in section 4. Altogether, respondents reported 85 prescribing errors during the interviews, including silly errors and ones felt by interviewees to be more serious, errors that had been deliberate (i. Reasons theory of error causation Reasons theory of error allowed some initial categorisation of errors. As outlined in Methods, the active failures of each incident were identified and classified as either knowledge-based errors, rule-based errors or the skill- based memory lapses and slips. Eighteen errors were mainly due to a knowledge-based mistake, 34 were due to a rule-based mistake, 23 were mainly due to slips or lapses and three were direct violations. A further seven incidents were related to receipt of incorrect information and therefore were not the active failure of the respondent but of another individual (these individuals included patients, nurses and other doctors). Therefore, these errors did not fit into one of Reasons categories and were given their own category, communication errors. The potential severity of prescribing errors ranged from minor errors, such as not signing a prescription to more serious errors such as prescribing penicillin to a patient who was allergic. A descriptive analysis of the common events leading up to each type of active failure is provided for each of them. These depict each active failure and its associated error- producing conditions and latent conditions (each individual error/critical incident has a unique number which can then be traced through the diagrams). These diagrams highlight one of our main findings, which was that errors were rarely due to a single causal factor, a finding which was consistent with the 2 results of our systematic review into the causes of prescribing errors. ure 4 depicts the various error producing conditions and latent conditions associated with 12 such slips, just one of which (incident number 44) impacted on a patient. Slips (12) Nurse 82,19,61,14 On call 76 Feeling Pressure from flustered 89,61 nurses 64 Covering lots of Pharmacist 3,1 wards 64 Doing >1 job at a time 64,62,44 A&E policy Start 44 Rushing 82,80,76,64, Unknown Start 61,44,27,14,3,1 patients 82, Understaffed 62 80,64,27,3 Workload 82,80,76, Wanting to go 64,61,44, home 82 27,14,3 Tired 80,64 Only paid for 48 hrs 27 Ignored E rxing warning 76 Not checking 82,44,14 Poor Design of E rxing communication system 76 with other Drs poor 80,46 Alert fatigue 76 Self 80,76,64,27,46 Others error/violation 46,80,14 44 ure 4: Factors implicated in the formation of skill-based slips. Two examples of errors are highlighted in the diagram by the red and green arrows (errors 44 and 64). The doctor quoted below described how he had made a slip by writing the dose of a drug in milligrams instead of micrograms, despite setting out to prescribe the latter; his only explanation was that he was in rush: It wasnt so much a mistake in what I wanted to write, but a mistake in what I wrote. So such as digoxin is something done in micrograms, and I know right in the beginning, erm, when I started prescribing, I knew it was micrograms, but... This error provoking condition was explored in greater detail with some interviewees; many felt that too many patients and not enough staff was the main reason for their excessive workload: …that team has far too, theres just, theres no way you can do that job from the allocated hours that they give.
Sensitization to a novel trigger for which there is lenges buy 20mg atorvastatin free shipping chart high cholesterol foods, administering oral immunotherapy cheap atorvastatin 5 mg line cholesterol qualitative test, and diagnosing and 108 discount 20 mg atorvastatin free shipping cholesterol test where to go,112 order atorvastatin 40 mg visa brown rice cholesterol lowering foods,134-141 no commercially available test allergen can be identified through treating anaphylaxis. A few of the studies have had a 137 a history of the event and confirmed by objective tests. Adverse effects have potentially include skin testing the patient and 1 or more controls been common with some oral immunotherapy dosing regimens, with crude extracts of the suspected culprit allergen (although especially on the initial dose escalation day and on subsequent 141 there is no quality assurance that such extracts contain the dose build-up days. This important gress will resolve the issue as to whether oral immunotherapy for screening test for mastocytosis reflects the increased burden of food-triggered anaphylaxis leads not only to clinical desensitiza- 78 mast cells in all forms of this disease. Insect venoms: allergen-specific immunotherapy (strength of recommendation 5 A) Medications : desensitization (strength of recommendation 5 B) Seminal fluid: desensitization (strength of recommendation 5 C) Idiopathic anaphylaxis (for frequent episodes only; strength of recommendation 5 C) Oral glucocorticoid, such as prednisone; H1-antihistamine, such as cetirizine (used for prophylaxis) Adapted from reference 153 and others; see text for details. Avoid the medications suspected of triggering anaphylaxis and substitute a non–cross-reacting medication, preferably from a different therapeutic class. Desensitization should be conducted in an appropri- allergens that trigger anaphylaxis might include allergen admin- ately equipped health care facility staffed by health care istration through the sublingual route, engineered recombinant professionals who are trained and experienced in using desensi- protein allergens, a mixture of major recombinant allergens, tization protocols and in the recognition and treatment of break- 34,144 CpG-oligonucleotide–conjugated allergens, peptides or polymers through symptoms, including those of anaphylaxis. Herbal Formula-2, a well-characterized mixture of Chinese herbs In patients with a history of vaccine- or vaccine component– that prevents food-induced anaphylaxis and leads to long-lasting triggered anaphylaxis who have negative skin tests to the vaccine immunologic tolerance in a murine model, has now entered and its components, it is highly unlikely that IgE antibody is 142 clinical trials. The vaccine can therefore be administered in the usual potentially provide an increased margin of protection against manner; however, it is prudent to observe such patients for food and other allergen triggers of anaphylaxis for many, although 1 hour afterward instead of the customary 30 minutes. For anaphylaxis triggered by a medication or a biological free seasonal influenza vaccine and egg-free pandemic A/H1N1 agent, avoidance is critically important. An alternative non–cross- vaccine grown in mammalian cell culture systems are now reacting agent, preferably from a different therapeutic class but available in some countries. If a suitable alternative vaccine is sometimes from the same class, can often be substituted effec- not available, the culprit vaccine should be administered in an 34 tively and safely. Where this is not possible, desensitization appropriately equipped and staffed health care facility by using a 34,144 48 with the offending agent is indicated. For anaphylaxis incremental manner over several hours have been published for triggered by stinging insects, avoidance of exposure involves some agents, such as b-lactam antibiotics or other antibiotics, as- several approaches. When outdoors, appropriate protective clothing, prophylaxis regimen involves 60 to 100 mg of prednisone each including shoes and socks, should be worn. Anti-IgE antibody injections have been reported to be laxis, a 3- to 5-year course of subcutaneous injections of the helpful in patients with idiopathic anaphylaxis and in anaphylaxis relevant standardized insect venom or venoms significantly with no apparent trigger that occurs in patients with mastocytosis. This potentially curative 53 Long-term risk reduction: Emergency preparedness treatment is underused. In children a 98% protection rate can be achieved, and the effect lasts for decades after venom injections for anaphylaxis recurrences in the community 52,145 are discontinued. Use of purified extracts potentially reduces Those at risk for anaphylaxis in the community and their 146 large local reactions during venom immunotherapy. Venom caregivers should be prepared to recognize episodes that occur immunotherapy can be safely administered to all those at risk, in- despite best efforts to avoid the relevant trigger and other cluding high-risk patients with mastocytosis or clonal mast cell preventive measures and to provide prompt life-saving first-aid 2,24-26,34,52,54,69,93,153 disorders, although a slow rate of dose escalation is often neces- treatment of such episodes. Anti-IgE antibody is reported to be paredness involves carrying 1 or more epinephrine autoinjectors, useful in controlling reactions to venom immunotherapy in pa- having an anaphylaxis emergency action plan, and wearing 149 1,2,24-26,54,69,153 tients with mastocytosis. For treatment of an anaphylaxis recurrence in the community, In adults venom immunotherapy significantly reduces sting- injection of epinephrine is the first-aid medication of choice, as induced cutaneous systemic reactions and is therefore indicated recommended in all anaphylaxis guidelines. The rationale for this 24,154,156-162 for patients with sting-induced generalized urticaria and no other is summarized in Table X. It also reduces large local reactions to mend injecting epinephrine from an autoinjector intramuscularly stings and might be considered for at-risk patients who cannot to- in the midanterolateral aspect of the thigh. The first aid dose of ep- tally avoid insect exposure, such as beekeepers, and/or those who inephrine is 0. This dose can 154,155,163-165 venom immunotherapy is not indicated either for sting-induced be repeated every 5 to 15 minutes, as needed. It de- vides short-term immunomodulation for patients at risk of creases mucosal edema, thereby preventing and relieving upper 59 anaphylaxis to seminal fluid. In the future, regular subcutaneous airway obstruction, and it also prevents and relieves hypotension 156-160 injections of anti-IgE antibody might be indicated for patients and shock (Table X). In addition, its b1-adrenergic effects with anaphylaxis triggered by various allergen triggers. In most countries the highest of exercise-induced anaphylaxis include strict avoidance of epinephrine dose currently available in an autoinjector is 0. Delayed injection of 18-21 extremes of temperature and humidity, and high pollen counts. After intramuscular injection into the vastus lateralis, absorption is rapid, and epinephrine reaches the central circulation rapidly. Rapid absorption is critical in anaphylaxis in which the median time to respiratory or cardiac arrest is 15 minutes (venom) to 30 minutes (food). Ideally, epinephrine doses should be stated concentrations (ie, milligrams per milliliter) rather than as ratios; however, both methods are in common use. It should be given only by physicians who are trained and experienced in the dose titration of vasopressors (preferably by using an infusion pump) against continuous hemodynamic monitoring. This action and the vasodilator effect in skeletal muscle produced by endogenous epinephrine are well-recognized aspects of the fight-or-flight response. Most the thigh to measure the distance from the skin to the surface of patients with anaphylaxis respond promptly to epinephrine injec- 170,171 the vastus lateralis muscle. Transient pharmacologic effects of epinephrine, such as pallor, Health care professionals need to be trained to use epinephrine tremor, anxiety, palpitations, headache, and dizziness, that occur autoinjectors correctly and safely in order to train and coach those within 5 to 10 minutes after injection are usually mild and confirm at risk for anaphylaxis and their caregivers in how to use them that a therapeutic epinephrine dose has been given. Unintentional injections from epinephrine effects, such as pulmonary edema or hypertension, are usually autoinjectors into fingers, thumbs, and hands by patients self-in- attributable to epinephrine overdose.
Probabilities of death at ages 0–34 and 35–69 generic 5 mg atorvastatin with visa cholesterol guidelines calculator, with probabilities of death from smoking at ages 35–69 shaded purchase 5mg atorvastatin with mastercard cholesterol in foods list. The full hazards of smoking and the benefits of stopping: cancer mortality and overall mortality 593 Table P7 purchase 5mg atorvastatin overnight delivery cholesterol in poultry eggs. Projected numbers of deaths from tobacco during the 21st century generic 40 mg atorvastatin visa cholesterol test edinburgh, if current smoking patterns persista Period (years) Deaths from tobacco (millions) 2000–2024 ~150 2025–2049 ~250–300 2050–2099 > 500 Total, entire 21st century ~1000 Total, entire 20th century ~100 aWorldwide, about 30% of young adults become smokers, and with the current low cessation rates among smokers in low- and middle-income countries, most who start will not stop. Tobacco is second half of the century, but not therefore expected to cause about Cessation before. In contrast, widely practica- 150 million deaths in the frst quar- If many of the adults who now smoke ble ways of helping large numbers ter of this century (many of which were to give up over the next decade have already happened, as smok- of adult smokers to quit (prefer- or two, thus halving global cigarette ing is already causing about 6 mil- ably before middle age, but also in consumption per adult by the 2020s, lion deaths a year worldwide [20]) middle age) could well avoid more this would prevent about one third and 250–300 million in the second than 100 million tobacco-related of tobacco-related deaths in the quarter. Predictions for the third deaths in the frst half of this cen- 2020s and almost halve tobacco- and, particularly, the fourth quarter related deaths thereafter. Large numbers of deaths dur- of the century are inevitably more decade of their occurrence, such ing the second half of the century speculative. However, due partly changes could avoid 10 or 20 million would also be avoided if many of to population growth and partly to tobacco-related deaths per decade, those who, despite everything, still the maturing of the epidemic, if cur- and could avoid 100 million tobacco- start to smoke in future years could rent smoking patterns persist then related deaths in the second quarter be helped to stop before they are the number of tobacco-attributed of the century. Such calculations deaths is likely to exceed 100 mil- suggest that the effect of quitting lion per decade throughout the sec- could be more rapidly apparent on Not starting ond half of the century (Table P7. Both, how- Cessation and not starting smoking by young people, the pro- ever, are of great importance. We are grateful to Jillian Boreham and less a substantial proportion of the of millions of deaths from tobacco Kirstin Pirie for help with the fgures. Mortality from smoking world- smoking and benefts of cessation in the demic on entering its second century. Impact of smoking on mortality cancer: quantitative estimates of avoid- factors and risk factor clusters in 21 re- and life expectancy in Japanese smok- gions, 1990–2010: a systematic analysis able risks of cancer in the United States ers: a prospective cohort study. The full hazards of smoking and the benefits of stopping: cancer mortality and overall mortality 595 Contributors Jean-Pierre Abastado Benjamin O. Baan Singapore Immunology Network University of Washington School of International Agency for Research Singapore Medicine on Cancer jean-pierre. Armstrong Case Comprehensive Cancer the University of Tokyo Sydney School of Public Health Center Tokyo, Japan the University of Sydney Case Western Reserve University akazah@med. Allen and University of Oxford Héctor Arreola-Ornelas Fundación Mexicana para la Salud Central Brain Tumor Registry of the Oxford, United Kingdom Mexico City, Mexico United States naomi. Chaloupka Cancer Council Victoria Heather Bryant University of Illinois at Chicago Carlton, Australia Canadian Partnership Against Ron. Cantor Taipei, Taiwan, China Centre Hospitalier Universitaire National Cancer Institute chencj@gate. Environmental Protection Karolinska Institute University of Calgary Agency, Integrated Risk Information Stockholm, Sweden Alberta Health Services – Cancer System joakim. Galloway the Ohio State University Medical Thimphu, Bhutan College of Life and Environmental Center Science doj08@yahoo. Gelderblom Imperial College London London, United Kingdom South African Medical Research Sarah C. Goodell University of Oxford Cancer Stem Cells and Regenerative Oxford, United Kingdom Toronto, Canada Medicine Center sarah. Michaels Hospital Public Health Institute on Cancer Dalla Lana School of Public Health Turkish Ministry of Health Lyon, France University of Toronto Ankara, Turkey vargash@iarc. Karagas Navi Mumbai, India School of Psychological Sciences Norris Cotton Cancer Center guptapc@healis. Pathology Senior Visiting Scientist at University of California San Diego International Agency for Research School of Medicine on Cancer James F. Humphrey Takanori Hattori Washington University School of Tim Key Shiga University of Medical Science Medicine University of Oxford Tokyo, Japan St. Lakhani Jonathan Liberman University of Queensland Centre for McCabe Centre for Law and Cancer Günter Klöppel Clinical Research Cancer Council Victoria and Department of Pathology the Royal Brisbane and Womens Union for International Cancer Technical University of Munich Control Munich, Germany Hospital Carlton, Australia Guenter. Lash Hospital del Mar Research Institute Joannie Lortet-Tieulent Wayne State University School of International Agency for Research Barcelona, Spain Medicine on Cancer kogevinas@creal. Odedina Regional Cancer Centre Union for International Cancer Pharmaceutical Outcomes and Trivandrum, India Control Policy beelasmathew@hotmail. McKay International Agency for Research Health Disparities, Shands Cancer on Cancer Raul Hernando Murillo Moreno Center Lyon, France Instituto Nacional de Cancerología University of Florida mckayj@iarc. Johan Offerhaus University Medical Center Utrecht Oscar Méndez Biomedical Sciences Utrecht, Netherlands Fundación Mexicana para la Salud Queens University Belfast g. Middleton on Cancer Richard Muwonge Warren Alpert Medical School of Lyon, France Brown University International Agency for Research ohgakih@iarc. Miller Fidele Ngabo Danish Cancer Society Dalla Lana School of Public Health Copenhagen, Denmark Ministry of Health of Rwanda University of Toronto jorgen@cancer. David Miller University of Oxford Carleton University Center for Research in Oxford, United Kingdom Ottawa, Canada Environmental Epidemiology hongchao. Riley Epidemiological Studies Unit Madras, India United States Department of University of Oxford drtrajkumar@gmail. Rath Group, Department of Health Cambridge, United Kingdom Department of Radiotherapy Sciences pp10001@medschl. Ray University of Franche-Comté International Agency for Research Healis, Sekhsaria Institute for Besançon, France on Cancer and Public Health Navi Mumbai, India Lyon, France Laboratory of Skin Bioengineering and Imaging raycs@healis. Sutcliffe International Agency for Research Ronald Simon Terry Fox Research Institute on Cancer University Medical Center Vancouver, Canada Lyon, France Hamburg-Eppendorf cci-cancercontrol@shaw.
The two characteristics of stem cells that distinguish them from all other cells are self-renewal and multi- potency cheap atorvastatin 20 mg on line cholesterol ratio by age. Self-renewal is the capacity of a cell to divide and produce identi- cal daughter cells over a long time period purchase atorvastatin 40 mg online cholesterol test in lab. Tumour cells can be els of cancer can be unifed 20 mg atorvastatin amex cholesterol levels in quinoa, two ing cheap 5mg atorvastatin with amex cholesterol test margin of error, and lentiviral lineage tracing, the genetically diverse due to mutations different studies were performed repopulation dynamics of many sin- and clonal evolution, resulting in in- examining cancer stem cells at both gle lentivirus-marked lineages from tratumour functional heterogeneity. Despite erogeneity due to epigenetic differ- tient samples had extensive sub- this genetic stability, the prolifera- ences; that is, all cells present after clonal genetic diversity, and through tion, persistence, and chemother- long-term tumour growth are derived the use of xenotransplant assays, from cancer stem cells. There is this diversity was established to have apy tolerance of lentivirus-marked strong evidence for the cancer stem originated from within the leukaemia- lineages were variable within each cell model in acute myeloid leukae- initiating cells. Stem cells are essential for of genetically modifed animal mod- so-called cancer stem cells resulted the development of each organism els, such as knockout mice, which in the cancer research community and thus can be considered to be a are essential in cancer research. Given human stem cells and, in particular, long been considered to be derived the potential of stem cells, their function and proliferation are sub- ject to a range of control processes. Genetic and epigenetic changes in susceptible cells may be an early event in the development of cancer and give rise to cancer stem cells and contribute to tumour Dysregulation of the surveillance heterogeneity. The origin of cancer stem cells may be early stem or progenitor cells, or mechanisms for proliferation and dif- differentiated cells distinguished by abnormal expression and function of a set of genes ferentiation of stem cells may initiate that may contribute to reprogramming into a pluripotent state. Cancer stem cells Stem cells were discovered more than 30 years ago and have been ex- ploited extensively for the generation 230 Table 3. Many cancers have been In addition to surface markers, initial events allow for the expansion found to contain cells with proper- cancer stem cells may share many of transformed cells and the forma- ties of stem cells. However, in most key properties with embryonic stem tion of a population of altered cells, cases the existence of cancer stem cells. These properties include in- or a clone, with the capacity to grow cells has been documented function- fnite proliferation potential and the and divide in defance of normal cel- ally: the presence of cancer stem capacity to invade tissues and or- lular control. Continuing selection of cells in the bulk of cancer cells is gans and to promote formation of ftter and more aggressive cells re- discerned by their capacity to form blood vessels for their own oxygen- sults in a generation of cancer clones tumours after transplantation into an ation. Therefore, cancer stem cells capable of invading and destroying immunocompromised animal host, may contribute to the heterogeneity neighbouring tissues and migrating most commonly a mouse. Although to distant organs to form metastatic assays reveal that only a small frac- important progress has been made tumours. The identity of that original tion of cancer cells are capable of in the identifcation of cancer stem target cell is not known . However, recent studies indicate that Importantly, these cells not only can Cancer stem cells are believed to many genetic and epigenetic chang- form tumours upon transplantation arise in different ways. First, cancer es underlying the aggressive and but also can recapitulate tumour het- stem cells can be derived from nor- destructive behaviour of cancer are erogeneity [9]. However, until very mal tissue-specifc stem cells as a orchestrated by a discrete population recently, the isolation of a cancer result of specifc genetic and epige- of cancer cells with stem cell proper- stem cell population using molecular netic changes that abrogate prolif- ties. These cells are known as cancer signatures, cell surface markers, or eration control in the normal cells. However, al- brid cells may be cancer-initiating organized into undifferentiated cells though some markers are common to cells with stem cell properties [32]. Cell reprogramming factors can induce pluripotent stem cells, with potential the discovery of stem cell mas- applications in therapy. This phenotypic reversal or de- differentiation essentially involves enabling specialized cells such as neurons or muscle fbres to regain stem cell properties, which would allow the generation of practically any type of cell. Such a scenario may solve important ethical issues associated with the use of embryos as a source of stem cells, as demon- strated by recent studies [3]. Several laboratories have demonstrated that the introduction of as few as four master genes into either human or murine differentiated cells mediates the emergence of stem cells. This remarkable phenomenon provides support for the argument that differ- exclusive, and the genesis of cancer cell pool may be rapidly depleted. Reprogramming can alter any cell of the body so that it may function as a pluripotent stem cell. Shown are human induced pluripotent stem cells derived cells have been known for many from dermal fibroblasts. Immunofluorescence analysis with an antibody against decades, the genetic basis of stem Nanog protein (red) is used to indicate that Nanog (a master transcription factor cell identity only began to be under- critically involved in stem cells and a widely used marker of the pluripotent state) is stood recently. With these methods, a limited number of genes have been discovered that are necessary and suffcient to maintain self-renewal and pluripotency – the two distin- guishing features of stem cells. These genes encode transcription factors that control the transcription of other genes . When the rel- evant genes are inactivated or mu- tated, stem cells may differentiate into specialized cells and the stem 232 . Conventional therapies may reduce tumour size by killing mainly differenti- Stem cells and cancer therapy ated tumour cells. If the putative cancer stem cells are less sensitive to these therapies, Much current interest in stem cells then cancer stem cells will remain viable after therapy and re-establish the tumour. By contrast, if therapies can be targeted against cancer stem cells, then they might more and cancer stem cells is predicated effectively kill the cancer stem cells, rendering the tumours unable to maintain them- on the realization that this tiny, yet selves or grow. Thus, even if cancer stem cell-directed therapies do not shrink tumours critical, population of cancer cells initially, they may eventually lead to cures. Many currently used protocols for cancer therapy are now under- stood to fail – marked by the reap- pearance of disease – due to an inability to eradicate cancer stem cells. Such a clinical course suggests that the ther- apy used specifcally targets rapidly growing tumour cells, whereas more slowly growing cancer stem cells may be spared. Thus, major challenges will be (i) to discover effcient ways to identify and isolate tissue-specifc cancer stem cells may also arise by of the same process. Conversely, stem cells and cancer stem cells, (ii) non-genetic changes that confer cells with established stemness to gain insights into the mechanisms certain features on differentiated features may acquire characteris- of self-renewal and pluripotency of cells. The normal stem cells and cancer stem by the knowledge that all cells, in- balance between stemness and a cluding stem cells, in any given or- cells, and (iii) to identify genetic and differentiated character appears to ganism share an identical genome.
Discount 5 mg atorvastatin. Cholesterol test kit | CURO L5 | How to pair CURO L5 & Test Strips.