
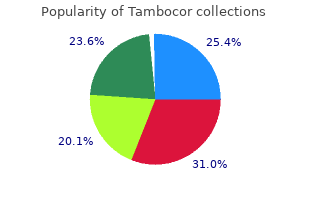
Tambocor
"Discount tambocor 50mg free shipping, medications quetiapine fumarate."
By: William A. Weiss, MD, PhD
- Professor, Neurology UCSF Weill Institute for Neurosciences, University of California, San Francisco, San Francisco, CA

https://profiles.ucsf.edu/william.weiss
The photosensitizer accumulates in the target cells and absorbs light of a certain wavelength 50 mg tambocor visa. The energy is transferred to discount tambocor 100 mg on line oxygen and highly reactive oxygen species discount 50mg tambocor with visa, mainly singlet oxygen 100mg tambocor visa, are generated. To date porphyrins, chlorine derivatives, or phthalocyanines have been studied for primary or adjuvant cancer therapy (2). The lesions were painted consecutively with eosin dye plus intratumoral injection of eosin and were then exposed to sunlight or light from a carbon arc lamp for six to eight hours a day. Depending on the subcellular localization of the photosensitizer, site-speci c damage occurs, thus leading to necrosis/apoptosis or modulation of cellular functions. As systemic photosensitizing drugs induce prolonged phototoxicity (3), topical photosensitizers are preferred for use in dermatology. Alternatively, the activated photosensitizer changes from 23 the singlet state into the more stable triplet state with a longer half-life period (10 seconds) (a process referred to as �intersystem crossing�). In the type-I photo-oxidative reaction, there is a direct hydrogen and electron transfer from the triplet state of the photosensitizer to a substrate. These radicals are able to react directly with molecular oxygen and form peroxides, hydroxy-radicals, and superoxide anions. Direct damage to the cells by this reaction can occur, especially when the photosensitizer is bound to easily oxidizable molecules. The highly reac tive state of singlet oxygen results in very effective oxidation of biological substrates. Both reac tion types can compete in parallel, as substrate and molecular oxygen compete for the photosensitizer in the triplet state. What kind of reaction preferably happens depends on the photosensitizer used, its subcellular localization, and the substrate, and oxygen supply around the activated photosensitizer. These small molecules easily penetrate the epidermis due to their low molecular weight w (2,7). If no surface illumina tion is given, the photoactive porphyrins are metabolized to the photodynamically inactive heme within the next 24 to 48 hours (2,7). Although topically applicable photosensitizers are most commonly used in dermatology, recent investigations have shown that the prolonged photosensitivity after systemic application of photosensitizers can be alleviated by chemical modi cation. Typically, ltered xenon arc sources or tungsten lament quartz halogen sources have been used with emission ranges between 600 and 700 nm. These have relatively narrow emission spectra with greater photosensitizer activation ef ciency and, therefore, lower dose requirements. In general, irradiances of less than 150 mW/cm are used to avoid hyperthermia, and indeed, the lower the irradiance, the less pain appears to occur with treatment and outcomes may be improved (17,21). Assessment of the site and maximum diameter of the lesion is necessary and photo graphic documentation may be helpful. Application of petrolatum or debriding agents to the lesion(s) for a few days prior to treatment may loosen surface crust or hyperkeratosis and, if heavy crusting is present, surface preparation with either a spatula or curette without local anesthetic is commonly practiced, although there is no evidence that this improves treatment outcomes. If the lesion is on a sunlight-exposed site, such as head and neck, an additional light-opaque dressing is required to protect the treatment site prior to irradiation. This can all be performed on an outpatient basis and the patient will then return for irradiation later that day (28). On the basis of naked eye and Wood�s light examination the irradiation eld is mapped out to include a 5 mm rim of clinically normal appearing tissue and the maximum diameter of the eld documented. Irradiation is performed with one of 2 several possible light sources, as discussed (Table 1). However, talking to patients to put them at ease, use of a cooling fan, xylocaine spray, and a Photodynamic Therapy 375 w device such as the Cynosure /Zimmer cold air blower, which delivers a jet of chilled air to the skin surface may be helpful. These changes are maximal during and immediately after irradiation and usually subside within 24 to 48 hours of treatment, although in ammation and crusting will occur over one to two weeks. Persistent erythema and hypo or hyper-pigmentation may occur at the treatment site for a few weeks after treatment, but usually resolve leaving no more than an extremely faint scar and excellent cosmetic outcome (35). However, the assessment of lesion responses by medical staff is strongly advised, as it may sometimes be dif cult to distinguish whether persistent erythema is representative of residual disease or merely the result of treatment. For illumination purposes, either blue light (417 nm) or red (635 nm) have been used (43,44). In 243 patients, clinical response, based on lesion clearance, was assessed at weeks 8 and 12. Moderate to severe discomfort during illumination was reported by at least 90% of patients; however, only 3% of patients required discontinuation of therapy (44). No difference was seen between the three incubation periods nor did pretreat ment with urea or lidocaine have an in uence on the therapeutic outcome (6). Two cycles of methyl aminolevulinate-photodynamic therapy (repetitive treatment after one week; three hours incubation; illumination with the Aktilite light emitting diode; 37 J/cm2). Cure rates reported so far are the best for all epithelial cancers or precursors (up to 100%). After one-year of follow-up, further recurrences reduced the complete clinical clearance rates to 82% and 42%, respectively (47). The former tumor areas were excised three months later and histopathologically evaluated for residual tumor. In the cryosurgery arm, lesions were treated with liquid nitrogen in the open spray technique using two freeze-thaw cycles for 25 to 30 seconds each time. The overall cure rate was 79%, cosmetic outcome was excellent or good in 98% of the completely responding lesions (49). The primary end point of this trial was the clinically assessed lesion clearance at three months after treatment, besides cosmetic outcome.
The white color (star) is � Occupational exposure secondary to 100 mg tambocor with amex trauma not regression purchase tambocor 100mg online. The brown (red � Medications (chemotherapeutic agents tambocor 100mg low cost, multiple nails) arrows) and purple blotches (white arrows) result from � Racial longitudinal melanonychia (multiple nails) the breakdown of blood buy 100mg tambocor with amex. No melanoma-specific criteria � Nail trauma or inflammation (nail biting, friction, are seen. This small papule was only found after Terminal hairs with perifollicular hypopigmentation a complete skin examination. There are different (boxes), pigment network (circles), and brown dots shades of pink color, pinpoint (boxes), and comma (arrows) characterize this small congenital melanocytic shaped vessels (yellow arrows) plus a milky red area nevus. Amelanotic melanoma and Merkel cell carcinoma are in the clinical and dermoscopic differential diagnosis. Asymmetry of color � Pink and structure (+), the multicomponent global pattern � Black pigment network (1, 2, 3) irregular brown globules (boxes), irregular � Atypical dark blotches (yellow arrows), and scar tissue (stars) � Spitzoid is the term used when any of the different with arborizing vessels (black arrows) characterize 6 patterns is seen this recurrent nevus. Review the original � Streaks and/or dots and globules at the periphery pathology report to confirm the benign nature of this � Light/dark brown, black, or blue color centrally lesion. There are a few streaks (red arrows) at all points of the periphery foci of irregular brown dots and globules (boxes), characterize this classic symmetrical starburst/Spitzoid irregular dark blotches (black arrows), and multifocal pattern. The � this can have any combination of melanoma hypopigmentation (black stars) should not be confused specific criteria similar to superficial spreading with regression. Following these, lesions with digital der criteria found on the trunk and extremities (Figs. This is a melanocytic lesion because it � Dermoscopy might not be as helpful to make the diag has aggregated brown globules (boxes). There is an nosis as the history of a melanoma being previously absence of melanoma-specific criteria found on the excised face with different shades of pink and brown color plus � Single or multiple ulceration (yellow arrows). Follicular openings (black � Pigmented and/or nonpigmented macules, papules, arrows) should not be confused with the milia-like and ulcerated or nonulcerated nodules can be seen in cysts of a seborrheic keratosis. However, this with dermoscopy set of clinical and dermoscopic features should raise a red flag for concern. Dermoscopy should not only be used on clinically suspicious lesions if one wants to diagnose melanoma incognito � Nail apparatus melanoma � Amelanotic reddish diffuse color/amelanotic tumor � Featureless melanoma � Diffuse melanonychia with different shades of black, � Melanoma without dermoscopic criteria at all brown, or gray color � Usually a pink or hypopigmented lesion � Irregular pigmented bands. Both can have pigmented and nonpig meet this criterion and can be found anywhere in the mented variants lesion � Dermoscopic features of solar lentigo, actinic kerato sis, and melanoma can be found in the same lesion Pearl � Multiple biopsies might be needed to make the correct the globules are the main dermoscopic feature used to diagnosis differentiate sebaceous gland hyperplasia from basal cell � Use the atypical features of melanoma when making carcinoma an incisional biopsy � Bowen disease (in situ squamous cell carcinoma) � Collision tumor � Usually solitary pink or reddish scaly macule, papule, � Lesion with the dermoscopic criteria for 2 different nodule, patch, plaque pathologies � On sun-exposed areas in elderly patients � Rarely one can find a triple collision lesion with 3 dif � Pinpoint and/or glomerular vessels ferent pathologies � Clusters and/or diffuse distribution of vessels through � Collision tumors are commonly seen out the lesion � Diagnostic criteria can be side by side or one can be � With or without homogeneous brown color and/or seen within the other dark dots and globules (pigmented Bowen disease) � Examples include � Seborrheic keratosis, basal cell carcinoma Pearls � Seborrheic keratosis, in situ or invasive squamous � Clinically and dermoscopically a pink scaly lesion with cell carcinoma pinpoint and/or glomerular vessels is not diagnostic of � Seborrheic keratosis, amelanotic, or pigmented Bowen disease. A rapidly � It is possible to see if the nits are full (vital nits) or empty growing nodule (arrow) representing a squamous cell which helps determine the success or failure of treatment carcinoma and the mountain and valley pattern of a seborrheic keratosis (box) characterize this lesion. The Pediculosis Pubis cobblestone pattern of a nevus is in the dermoscopic It is possible to easily see the parasite attached to adjacent differential diagnosis. Pigment network, brown globules, homogeneous blue fibrosing alopecia, discoid lupus, folliculitis decalvans) color, or parallel patterns � Decreased hair density � Pinpoint white dots (follicular and acrosyringeal openings) 2. Diagnosing a melanocytic lesion by default means that: � Loss of follicular openings A. There are high-risk criteria at the periphery of the � Cicatricial white patches lesion that are hard to identify. There are criteria for a seborrheic keratosis or basal Congenital Hair Shaft Abnormalities cell carcinoma associated with pigment network and Monilethrix brown globules. There is an absence of criteria to diagnose a melano � Elliptical nodes (normal shaft diameter) cytic lesion, seborrheic keratosis, dermatofibroma, � Narrow internodes (dystrophic hairs) pyogenic granuloma, or ink spot lentigo; therefore, � Elliptical nodes regularly separated by narrow internodes the lesion should be considered melanocytic. There is an absence of criteria to diagnose a mela � Hair shafts bend regularly at multiple locations in different nocytic lesion, seborrheic keratosis, basal cell carci directions noma, dermatofibroma, or hemangioma; therefore, � Trichorrhexis invaginata (�bamboo hair�) the lesion should be considered melanocytic. Which criteria can be used to diagnose a seborrheic � Invagination of the distal portion of the hair shaft into keratosis Milky red areas, irregular streaks, and pigmented fol � Bamboo/golf tee/matchstick hairs licular openings B. Furrows, ridges, sharp border demarcation, milia-like � Alternating light and dark bands are seen clinically cysts, pseudofollicular openings, fat fingers, and hair � Light bands represent air-filled cavities pin vessels D. Diffuse brown color, glomerular vessels, and milia � Flattened hair shafts like cysts � Twisting at irregular intervals 4. Which criteria can be used to diagnose a basal cell Pili trianGuli anD CanaliCuli carcinoma Arborizing and pinpoint vessels plus multifocal � Flattened hairs with longitudinal groves hypopigmentation Pili bifurCati anD MultiGeMini C. The absence of a pigment network, arborizing vessels, pigmentation, ulceration, spoke-wheel structures � Hair shafts grow from the same papilla D. Glomerular vessels, ulceration, and blue ovoid nests � Split from a single tip of pigmentation � Double tip (bifurcati) E. Islands of black blotches, arborizing vessels, and � Several tips (multigemini) moth-eaten borders 5. A variable number of red, sharply demarcated vascu lar spaces called lacunae and fibrous septae 1. Pigment network, arborizing vessels, and central specific criteria such as symmetry of color and white patch structure and one prominent color. Usually they have several well-developed melanoma periphery specific criteria such as asymmetry of color and C. A central white patch and peripheral pigment structure, multicomponent global pattern, regular network network, regular globules, and regular streaks.
All patients with known or suspected coronary disease should be taking aspirin unless contraindicated purchase 50 mg tambocor with amex. There is recent evidence that crushing prasugrel leads to generic 100 mg tambocor fast delivery faster drug absorption tambocor 100 mg with amex, and consequently buy cheap tambocor 100 mg online, more prompt and potent antiplatelet effects compared with whole tablet ingestion. A weakness of the trial was that the loading dose of clopidogrel in the comparison group was 300 mg whereas most recommendations 30 now are that the loading dose of clopidogrel should be 600 mg. Nevertheless, particular benefit is apparent in patients with diabetes and those under the age of 75. Consideration should be given to administering clopidogrel at a dose of 150 mg for the first week and then 75 mg (31) daily. Duration will usually be for 12 months regardless of the stent deployed, but check with the consultant responsible. Some retrospective studies had raised concerns 35;36 that such treatment might reduce the cardiovascular efficacy of clopidogrel. A randomised controlled trial of 3627 patients taking aspirin and clopidogrel randomised to omeprazole or placebo found no difference in vascular outcomes 37 38;39 between groups. Patients on warfarin who require aspirin and clopidogrel therapy should be discussed at consultant level before any antiplatelet platelet or anticoagulation medication is discontinued. Management decisions need to be made on a case-by case basis (see later �triple anticoagulation� page 59). It confirmed a significant improvement of combined clinical endpoints including mortality. Restoration of normal flow in the culprit artery 42-45 is achieved in over 95% in most studies with significant long-term benefits. If it is likely that delay to treatment is going to be greater than 2 hours serious consideration should be given 46 to administration of a lytic agent. In office hours patients should be taken directly to the catheter lab and an assessment made en route. An effort should be made to document timings as follows: time of onset of symptoms, time of call for help, time of crew arrival and time of arrival in hospital and time of arrival in the lab. Patients should be administered aspirin and prasugrel (or clopidogrel or ticagrelor) as outlined previously (page 49). Patients should be assessed carefully after procedures for signs of bleeding, especially from sites of vascular access. Groin complications are not uncommon and imaging with ultrasound may be indicated to exclude false aneurysms etc. Vascular complications from radial procedures are unusual but patients must still be assessed carefully. Patients are pre-alerted by the paramedic crews and cardiology anaesthetic teams are activated. Blood gases should be obtained as soon as possible but this should not delay the undertaking of the angiogram as gases can be obtained after vascular access has been achieved. A tiny proportion of patients will however have received thrombolysis by a referring hospital. Patients should be aware that there is a 0�5% risk of major haemorrhagic complications, including stroke. Bleeding Problems after Thrombolytic Therapy the major serious complication associated with thrombolysis is haemorrhage and, if intracranial, this may be fatal. This data is based on mortality statistics however, rather than angiographic findings. Overall, the changes are not sensitive and specific enough for (55) clinical purposes. Patients within 6 hours of myocardial infarction are those most likely to benefit. In patients presenting days after the acute event with Q waves, only patients with recurrent angina and/or documented ischaemia with proven viability benefit from revascularisation. Management includes the use of intracoronary isosorbide dinitrate (1 2 mg boluses) adenosine (30 60 �g) or verapamil (0�5 1�0 mg). In the absence of persistent pain or haemodynamic 67 deterioration, a waiting period of 3 7 days appears to be the best compromise. There is good evidence that early (26;68) blocker therapy is beneficial, although patients with extensive myocardial infarction and a bradycardia may deteriorate. Benefit is probably greater if blockade is given early and is possibly due to a reduction in cardiac rupture on day one. They should still be considered prior to discharge in patients who have had transient failure. In patients who have received thrombolysis, diltiazem may reduce further non-fatal events and the need for revascularisation, but does not (72) appear to impact on mortality. The dihydropyridine group of calcium antagonists (nifedipine, nicardipine, amlodipine, lercanidipine, felodipine) should generally not be used after myocardial infarction and may cause adverse effects. They are also useful in patients with heart failure following myocardial infarction and in the management of hypertension in the setting of myocardial infarction. Care should be taken in patients with suspected right ventricular infarction as giving nitrates may result in hypotension. Studies have also suggested a reduction in late cardiac failure, myocardial infarction 73-76 and death. There is now evidence that all cardiac patients, regardless of the cholesterol level, benefit from statin therapy.
Syndromes
- Speech impairment
- Time stung
- This surgery usually takes about 1 hour. There is much less blood loss with this kind of surgery.
- The cornea is the clear (transparent) tissue covering the front of the eye.
- How to eat a heart-healthy diet
- Hyperkalemia
It is important to discount 50 mg tambocor with mastercard distinguish pre-syncope from dizziness (vertigo) as patients may mean different things when they complain of dizziness order tambocor 50mg on line. It is important to generic tambocor 50mg otc establish what happened before purchase tambocor 50 mg otc, during and after the syncopal episode. There are recent guidelines on the 201 investigation and management of syncope from 2018. There are different types of syncope: reflex or neurally mediated syncope, orthostatic hypotension and cardiac arrhythmia syncope. Neurally mediated syncope is often associated with prodromal symptoms (feeling hot, sweating, light-headedness, visual changes). On regaining consciousness there is usually rapid recovery with no drowsiness, confusion or headache. The most common type of neurally mediated syncope is neurocardiogenic (vasovagal) syncope. Other neurally mediated syncopal conditions include carotid sinus syndrome or syncope after urination, defaecation, swallowing or coughing (�situational� syncope). A simple faint can be categorised by the 6 P�s: Posture (prolonged standing or sitting), Provoking factors (pain, fear), Prodromal symptoms, Post-syncope nausea or vomiting, Post recovery recurrence syncope provoked by sitting or standing, Previous episodes. Advice needs to include avoidance of triggers, ensuring adequate hydration, limiting alcohol etc. Orthostatic syncope occurs when there is insufficient vasoconstriction in response to orthostatic stress (standing). Cardiac syncope refers to the conditions where syncope is caused by a decrease in cardiac output due to a primary cardiac aetiology. Where a cardiac cause is thought to be very likely (see above) admission may be indicated. The appropriate type of recording and length needed should be gauged by the frequency of events. The bulk of arrhythmia-related syncope detected by loop recorders are bradycardias, especially in the elderly. This is performed under local anaesthesia and enables correlation of clinical events to cardiac rhythm. Electrophysiology studies are underutilised generally in the investigation of syncope but the diagnostic yield is quite high. Tilt studies are generally indicated in patients with frequent episodes of syncope where an arrhythmia is felt to be unlikely. In patients over the age of 40, carotid sinus hypersensitivity should be considered. Management of neurocardiogenic syncope includes patient education, lifestyle changes and physical counterpressure manoeuvres. Avoidance of triggers (prolonged standing, moving from lying/sitting to standing quickly, hot baths/showers, fasting, excessive alcohol intake or drugs with vasodepressor properties) and ensuring adequate salt and fluid intake may reduce syncope frequency. Common physical counterpressure manoeuvres include leg crossing, limb and/or abdominal contraction, isometric arm contraction, bending forward, squatting, toe raising and knee flexion. The most effective and least cumbersome appears to be leg crossing and whole body muscle tensing in an attempt to mitigate the blood pooling to prevent syncope. Further interventions such as an increase in salt and water, tilt training, head-up sleeping, abdominal binders, elastic stockings and medical therapy are considered for recurrent neurocardiogenic syncope. It is recommended that patients with recurrent neurocardiogenic syncope drink 2 3 litres of fluid per day or enough fluid to avoid dark urine and ingest 10 g of salt per day. Management of orthostatic hypotension includes education and the maintenance of adequate fluid and salt intake. In patients without underlying hypertension, 2�3 litres of fluid and 10 g of salt per day is recommended to expand extracellular volume. In patients with drug induced autonomic failure, removal of the offending agent, when possible, is recommended. Although trial data is lacking, pacing is indicated in carotid sinus hypersensitivity. The recommended treatment is dictated by the risk of syncope recurrence, risk of cardiac arrest and efficacy of the treatment. Some will be post-viral, but post-partum cardiomyopathy and alcohol abuse also need to be considered. Treatment, whenever possible, should also be aimed at the underlying disease (if identifiable). Many patients with clinical features of heart failure however have echocardiograms that suggest just mild impairment or even normal systolic function. It is important to consider and exclude other causes such as coronary artery disease, pulmonary disease, anaemia etc. Nonetheless these patients have mortality similar to patients with left ventricular dysfunction and are equally disabled. Most patients with systolic heart failure will have underlying coronary artery disease, but a fair proportion will have a non-ischaemic cardiomyopathy. Patients who are admitted with a diagnosis of heart failure have a high mortality, both as inpatients (up to 10%) and following discharge (up to 50% in the following 12 months). Routine blood tests Renal function should be assessed to give clues as to previous hypertension, effect of medication and baseline. A careful family history (see later) is important to identify familial disease and genetic testing should be seriously considered.
Purchase tambocor 50 mg without a prescription. Pastilla amarilla para hombres - Tadalafil | Indicaciones y riesgos | Erección disfunción Eréctil.