
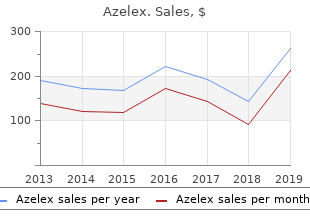
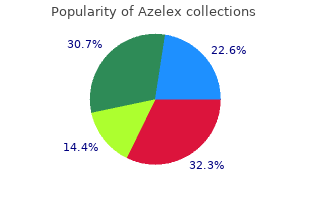
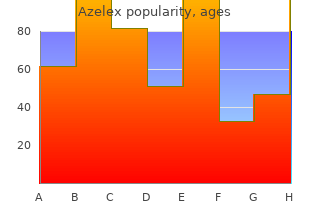
Azelex
"Discount 15g azelex overnight delivery, treatment of gout."
By: William A. Weiss, MD, PhD
- Professor, Neurology UCSF Weill Institute for Neurosciences, University of California, San Francisco, San Francisco, CA

https://profiles.ucsf.edu/william.weiss
Ensure that a colorectal surgeon gives any person who is considering surgery (and their family members or carers as appropriate) specific information about what they can expect in the short and long term after surgery discount azelex 15g with mastercard, and discusses this with them cheap azelex 15g otc. Maintaining remission in people with ulcerative colitis Proctitis and proctosigmoiditis 27 buy 15g azelex visa. To maintain remission after a mild to 15g azelex with mastercard moderate inflammatory exacerbation of proctitis or proctosigmoiditis, consider the following options, taking into account the person�s preferences: r � a topical aminosalicylate alone (daily or intermittent) or s r � an oral aminosalicylate plus a topical aminosalicylate (daily or intermittent) or s � an oral aminosalicylate alone, explaining that this may not be as effective as combined treatment or an intermittent topical aminosalicylate alone. Consider oral azathioprine or oral mercaptopurine to maintain remission: � after two or more inflammatory exacerbations in 12 months that require treatment with systemic corticosteroids or � if remission is not maintained by aminosalicylates. The prescriber should follow relevant professional guidance, taking full responsibility for the decision. To maintain remission after a single episode of acute severe ulcerative colitis: u u � consider oral azathioprine or oral mercaptopurine � consider oral aminosalicylates in people who cannot tolerate or who decline azathioprine and/or mercaptopurine, or in whom azathioprine and/or mercaptopurine are contraindicated. Consider a once-daily dosing regimen for oral aminosalicylates when used for maintaining remission. Take into account the person�s preferences, and explain that once-daily dosing can be more effective, but may result in more side effects. When caring for a pregnant woman with ulcerative colitis: � Ensure effective communication and information-sharing across specialties (for example, primary care, obstetrics and gynaecology, and gastroenterology). Include information relevant to a potential admission for an acute severe inflammatory exacerbation. Consider monitoring bone health in children and young people with ulcerative colitis in the following circumstances: � during chronic active disease � after treatment with systemic corticosteroids � after recurrent active disease. Monitor the height and body weight of children and young people with ulcerative colitis against expected values on centile charts (and/or z scores) at the following intervals according to disease activity: � every 3�6 months: o if they have an inflammatory exacerbation and are approaching or undergoing puberty or o if there is chronic active disease or o if they are being treated with systemic corticosteroids � every 6 months during pubertal growth if the disease is inactive � every 12 months if none of the criteria above are met. Consider referral to a secondary care paediatrician for pubertal assessment and investigation of the underlying cause if a young person with ulcerative colitis: � has slow pubertal progress or � has not developed pubertal features appropriate for their age. What is the clinical and cost effectiveness of prednisolone compared with aminosalicylates for the induction of remission for people with moderate ulcerative colitisfi What is the clinical and cost effectiveness of prednisolone plus an aminosalicylate compared with beclometasone plus an aminosalicylate for induction of remission for people with moderate ulcerative colitisfi What are the benefits, risks and cost effectiveness of methotrexate, ciclosporin, tacrolimus, adalimumab and infliximab compared with each other and with placebo for induction of remission for people with subacute ulcerative colitis that is refractory to systemic corticosteroidsfi What is the clinical and cost effectiveness of regular maintenance treatment compared with no regular treatment (but rapid standard treatment if a relapse occurs) in specific populations with mild to moderate ulcerative colitisfi To develop and validate a risk tool that predicts the likelihood of needing surgery for adults admitted to hospital with acute severe ulcerative colitis. All recommendations relate to adults, children and young people unless specified otherwise. These terms are defined as follows: � adults: 18 years or older � children: 11 years or younger � young people: 12 to 17 years. Severity of ulcerative colitis Mild, moderate and severe In this guideline, the categories of mild, moderate and severe are used to describe ulcerative colitis: � In adults these categories are based on the Truelove and Witts� severity index (see Table 8). Table 8: Truelove and Witts� severity index Mild Moderate Severe Bowel movements Fewer than 4 4�6 6 or more plus at least (no. Rectal bleeding None 0 Small amount only, in less than 50% of stools 10 Small amount with most stools 20 Large amount (50% of the stool content) 30 3. Stool consistency of most stools Formed 0 Partially formed 5 Completely unformed 10 4. Inflammation affecting the rectum alone may be referred to as proctitis; proctosigmoiditis if the rectum and sigmoid colon are affected; left-sided colitis if the inflammation extends proximally from the rectum to no further than the splenic flexure; sub-total colitis if the inflammation extends beyond the splenic flexure, but does not affect the whole colon; total colitis, or pan-colitis, if the entire colon is affected. The natural course of ulcerative colitis is characterised by periods where symptoms are present, interspersed with periods of clinical remission. Mild attacks are defined as those where the stool frequency is less than four times per day, with only small amounts of blood. Treatment of these exacerbations � induction of remission � may involve a range of different drug types, administered by different routes and at different doses. These include: � choice of drug � site and mechanism of drug release � for orally administered 5-aminosalicylic acid preparations � route of administration � which may include combinations of different routes (eg oral and rectal administration) � dose. There are also patient-related factors which may influence the choice of treatment for induction of remission, which would include: � clinical severity of the exacerbation � extent of inflammation � patient preference � dosing regimens, for example, those which may enhance adherence to treatment. The most widely used drugs in this situation are corticosteroids and aminosalicylate preparations of which 5-aminosalicylic acid is the active moiety. Depending on the preparation, 5-aminosalicylic acid is released through differing mechanisms including loss of integrity of an outer coating or cleavage of a diazo bond from a pro-drug. The aim of this release, in people with ulcerative colitis, is to deliver adequate levels of 5-aminosalicylic acid to the colon and rectum. Systemically bioavailable corticosteroids, such as prednisolone, have been widely used, but concern remains about their side effects. Orally administered beclometasone has topical mucosal activity, but is extensively metabolised with less systemic bioavailability. Immunomodulator drugs (azathioprine, mercaptopurine, ciclosporin, tacrolimus and methotrexate) are also used. There is considerable variation and debate about appropriate outcome measures in studies examining induction of remission. Acute severe ulcerative colitis is regarded as a medical emergency and requires hospital admission for intravenous corticosteroids and prophylaxis against venous thromboembolism. Evidence relating to the use of systemic corticosteroids and ciclosporin was reviewed in this chapter. Parameters that would help in assessing response, and in selecting patients at higher risk of colectomy (and therefore who may benefit from escalation of medical therapy), are examined in detail in section 5. A cross in the box indicates evidence was found and the evidence has been reviewed in this chapter an empty box indicates no evidence was found. Ulcerative colitis Inducing remission in people with ulcerative colitis the reviews for the induction of remission in people with mild to moderate ulcerative colitis are presented in the following order: � Topical aminosalicylates (section 5.
For example buy azelex 15g visa, because of your medi cal condition buy 15g azelex otc, you pay a visiting nurse $300 per week for Physical Examination medical and household services buy discount azelex 15g on line. She spends 10% of her time doing household services such as washing dishes You can include in medical expenses the amount you pay and laundry buy 15g azelex visa. You can include only $270 per week as med for an annual physical examination and diagnostic tests ical expenses. See Pregnancy Test Kit Maintenance and personal care services under Long-Term Care, earlier. Additionally, certain expenses You can include in medical expenses the amount you pay for household services or for the care of a qualifying indi to purchase a pregnancy test kit to determine if you are vidual incurred to allow you to work may qualify for the pregnant. Then divide that cost in the same health insurance premiums paid by or through the pre manner as in the preceding paragraph. This includes extra rent or utilities you any amount of advance payments of the premium tax Page 12 Publication 502 (2019) credit that you did have to pay back can be included in primary reason for attending the school, and any ordinary medical expenses. The � Teaching Braille to a visually impaired person, cost of her health insurance premiums in 2019 is $8,700. Advance payments of the premium tax credit of $4,200 � Teaching lip reading to a hearing disabled person, or are made to the insurance company and Amy pays premi � Giving remedial language training to correct a condi ums of $4,500. Amy is treated as paying $5,100 ($8,700 ing a child with behavioral problems to a school where the less the allowed premium tax credit of $3,600) for health course of study and the disciplinary methods have a ben insurance premiums in 2019. The facts are the same as in Example 1, except Amy is allowed a premium tax credit of $4,900 on Sterilization her tax return and receives a net premium tax credit of $700. Amy is treated as paying $3,800 ($8,700 less the al You can include in medical expenses the cost of a legal lowed premium tax credit of $4,900) for health insurance sterilization (a legally performed operation to make a per premiums in 2019. Stop-Smoking Programs Prosthesis You can include in medical expenses amounts you pay for See Artificial Limb and Breast Reconstruction Surgery, a program to stop smoking. This includes the cost of supporting a mentally ill dependent at a specially equipped medical See Operations, earlier. Telephone Psychoanalysis You can include in medical expenses the cost of special telephone equipment that lets a person who is deaf, hard You can include in medical expenses payments for psy of hearing, or has a speech disability communicate over a choanalysis. Psychologist Television You can include in medical expenses amounts you pay to You can include in medical expenses the cost of equip a psychologist for medical care. It may Special Education also be the part of the cost of a specially equipped televi sion that exceeds the cost of the same model regular tele You can include in medical expenses fees you pay on a vision set. You can include in medical expenses amounts you pay for therapy received as medical treatment. You can include in medical expenses the cost (tuition, meals, and lodging) of attending a school that furnishes special education to help a child to overcome learning dis abilities. Overcoming the learning disabilities must be the Publication 502 (2019) Page 13 Transplants � Travel for purely personal reasons to another city for an operation or other medical care. You can include any expenses you pay for the medical care of a donor in connection with the donation of an or gan to you, your spouse, or dependent. You can include in medical expenses amounts you pay for transportation to another city if the trip is primarily for, and Transportation essential to, receiving medical services. You You can include in medical expenses amounts paid for can include lodging for a person traveling with the person transportation primarily for, and essential to, medical care. For example, if a parent is You can include: traveling with a sick child, up to $100 per night can be in cluded as a medical expense for lodging. However, see Medical ment required by a patient who is traveling to get med Conferences, earlier. However, you can include you can use the standard medical mileage rate of 20 charges for a health plan included in a lump-sum tuition cents a mile. He wants to figure the amount he can include in medical expenses both ways to see Vision Correction Surgery which gives him the greater deduction. He You can include in medical expenses amounts you pay to then adds the $100 tolls and parking for a total of $660. This includes fees you pay for member than the $530 he figured using actual expenses. You can include in medical expenses the amounts you pay for a wheelchair used for the relief of a sickness or Example. The cost of operating and maintaining the moves a breast as part of treatment for cancer. The surgery to recon struct the breast corrects a deformity directly related to the Wig disease. You can include in medical expenses the cost of a wig purchased upon the advice of a physician for the mental Dancing Lessons health of a patient who has lost all of his or her hair from disease. You can include in medical expenses amounts you pay for X-rays for medical reasons. For example, you can for health insurance you use in figuring your health cover include the cost of a prescribed drug the Food and Drug age tax credit. For more information, see the Instructions Administration announces can be legally imported by indi for Form 8885. You can include the cost of a prescribed drug you pur Health Savings Accounts chase and consume in another country if the drug is legal in both the other country and the United States. You can�t include in medical expenses amounts you con tribute to a health savings account.
If you experience any distress during the completion of this survey azelex 15g low price, please stop and seek assistance immediately through your employee assistance program or by contacting the local Burke Center azelex 15g overnight delivery. As this study was reviewed as exempt azelex 15g without a prescription, no further reporting is required unless you change the protocol or personnel involved buy azelex 15g free shipping. This email will serve as notice that your study has been reviewed unless a more formal letter is needed. Participants in a Pilot Training for Trainers in September 2012 also provided valuable feedback on the Toolkit: Lynn Amabile, Maureen Auger, Giovanni Billings, Chris Bray, Adam Brown, Julie Collins, Toni Chance, Theresa Chavez, Laurie Elliott, Susan Erstling, Kendra Gent, Evelin Gomez, Steven Grilli, Jane Halladay Goldman, Marla Himmeger, Susan Holl, Mary Kay Jankowski, Megan Johnson, Katie Kammerzell, Sarah Kelly-Palmer, Jennifer Koch-Zapfel, Kenneth Kurl, Becky Lieb Kennedy, Dawn Lewis-Cummings, Meghan Lukasik, Derek Luke, Holly Magana, Catherine Meister, Thad Paul, Donna Pence, Kristi Petersen, Ann Scheuermann, Elizabeth Sharda, Christine Siegfried, Kathie Snell, Kelly Sullivan, and Tanya Toyer. Suggested Citation Child Welfare Committee, National Child Traumatic Stress Network. Trauma can have a lasting impact on the well-being and functioning of these children and their families. For child welfare workers, the ability to understand the effects of trauma on the children and families whom they serve, and to identify and address the specifc trauma related needs of those children and families, is critical to effective case planning and improving the child�s overall life trajectory. This Comprehensive Guide, which is designed as a companion to the Child Welfare Trauma Training Toolkit�s Trainer�s Guide and Participant Manual, includes: n the defnition of a trauma-informed child welfare system n An overview of child traumatic stress and its varying impact on children n the Essential Elements of a Trauma-Informed Child Welfare System n Practical strategies that child welfare professionals can use with children and families in the system who have experienced trauma. By understanding how trauma impacts children, and adopting a trauma-informed child welfare practice approach, child welfare workers can play a crucial role in mitigating both the short and long-term effects of trauma and in ultimately improving the lives of the children they serve. Defnition of a Trauma-Informed Child and Family Service System While the effects of trauma are often prevalent and far-reaching among children in the child welfare system and can impact casework practice at multiple levels, trauma and its effects have historically been overlooked or not well understood in day-to-day child welfare practice. As a result, many children who have experienced trauma may not receive the types of support and services that are necessary to help them achieve safety, permanency, and well being. On the contrary, child welfare agencies may inadvertently participate in actions that exacerbate a child�s trauma, such as multiple placements or removing a child from his/her community or school. Researchers have identifed the need to apply a trauma-informed approach across child serving systems, such as child welfare, juvenile justice, education, and others. The article also provided recommendations for how to make each of these service systems more trauma-informed (Ko et al. Adopting a trauma-informed approach to child-serving systems provides benefts on multiple levels. It equips front-line workers, supervisors, and administrators with the tools and skills necessary to help children and families overcome trauma and manage their own secondary traumatic stress. It also provides a framework for educating the workforce and affliated stakeholders on the impact of trauma, and provides them with strategies to manage children�s diffcult behaviors and overwhelming emotions and ensure that children receive the services they need. The National Child Traumatic Stress Network�s trauma-informed service system workgroup collaboratively developed the following defnition of a trauma-informed child and family service system. A service system with a trauma-informed perspective is one in which programs, agencies, and service providers: (1) routinely screen for trauma exposure and related symptoms; (2) use culturally appropriate evidence-based assessment and treatment for traumatic stress and associated mental health symptoms; (3) make resources available to children, families, and providers on trauma exposure, its impact, and treatment; (4) engage in efforts to strengthen the resilience and protective factors of children and families impacted by and vulnerable to trauma; (5) address parent and caregiver trauma and its impact on the family system; (6) emphasize continuity of care and collaboration across child-service systems; and (7) maintain an environment of care for staff that addresses, minimizes, and treats secondary traumatic stress, and that increases staff resilience. As stated in the Adoption and Safe Families Act of 1997, the national goals for children in the child welfare system are safety, permanency, and well-being. For children with a history of trauma, such goals can be particularly diffcult to achieve. Safety: Trauma can adversely impact the child�s ability to protect himself/herself from abuse, or for the agency to do so, in at least the following ways: n the child�s inability to regulate moods and behavior may overwhelm or anger caregivers to the point of increased risk of abuse or revictimization. Permanency: Trauma reactions can adversely impact the child�s stability at home or in out-of home care. Well-being: Trauma may have both short and long-term consequences for the child�s mental health, physical health, relational capacity, functioning, and life trajectory. Child Welfare Trauma Training Toolkit: Comprehensive Guide�3rd Edition 7 January 2013 n A child�s traumatic experiences may alter his or her worldview so that the child now sees the world as untrustworthy and isolates himself/herself from family, peers, as well as social and emotional support. The Essential Elements of a Trauma-Informed Child Welfare System Child welfare is charged with integrating multiple systems in the child�s life in order to provide comprehensive and consistent services. While certain Essential Elements may be addressed by professionals in other systems, such as mental health or schools, it is the child welfare worker who coordinates with other systems to ensure that the child�s and the family�s trauma-related needs are being met. These Essential Elements are the province of all professionals who work in and with the child welfare system. They span investigation, child protection, ongoing service provision and coordination, court decision-making, and permanency. Implementation of each Essential Element must take into consideration the child�s developmental level and be responsive to the child�s family, culture, and language. Partner with agencies and systems that interact with children and families 8 the National Child Traumatic Stress Network The event overwhelms the child�s ability to cope and causes feelings of fear, helplessness, or horror, which may be expressed by disorganized or agitated behavior. Situations that may be considered traumatic include the following: n Physical or sexual abuse n Abandonment, betrayal of trust (such as abuse by a caregiver), or neglect n the death or loss of a loved one n Life-threatening illness of a caregiver n Witnessing domestic violence n An automobile accident or other serious accidents n Bullying n Life-threatening health situations and/or painful medical procedures n Witnessing or experiencing community violence. An earthquake, dog bite, or motor vehicle accident are all examples of acute traumas. Other examples include: n School shootings n Gang-related incidents n Terrorist attacks n Natural disasters. As the event unfolds, the child�s increased heart rate, overwhelming emotions, and other physical reactions can add to his or her fright and sense of being overwhelmed. Chronic trauma When a child has experienced multiple traumatic events, the term chronic trauma is used. Chronic trauma may refer to multiple and varied events�such as a child who is exposed to domestic violence, is involved in a serious car accident, and then becomes a victim of community violence�or longstanding trauma such as physical abuse or war. The effects of chronic trauma are often cumulative, as each event serves to remind the child of prior trauma and reinforce its negative impact. A child exposed to a series of traumas may become more overwhelmed by each subsequent event and more convinced that the world is not a safe place. Over time, a child who has felt overwhelmed over and over again may become more vulnerable to and less able to tolerate ordinary everyday stress.
Over a period of at least 6 months generic 15g azelex with mastercard, recurrent and intense sexual arousal from touching or rubbing against a nonconsenting person azelex 15g discount, as manifested by fantasies purchase azelex 15g with mastercard, urges buy discount azelex 15g on-line, or be� haviors. Specify if: In a controlled environment: this specifier is primarily applicable to individuals living in institutional or other settings where opportunities to touch or rub against a noncon� senting person are restricted. In full remission: the individual has not acted on the urges with a nonconsenting per� son, and there has been no distress or impairment in social, occupational, or other ar� eas of functioning, for at least 5 years while in an uncontrolled environment. Specifiers the "in remission" specifier does not address the continued presence or absence of frot teurism per se, which may still be present after behaviors and distress have remitted. Diagnostic Features the diagnostic criteria for frotteuristic disorder can apply both to individuals who relatively freely disclose this paraphilia and to those who firmly deny any sexual attraction from touch� ing or rubbing against a nonconsenting individual regardless of considerable objective evi� dence to the contrary. If disclosing individuals also report psychosocial impairment due to their sexual preferences for touching or rubbing against a nonconsenting individual, they could be diagnosed with frotteuristic disorder. In contrast, if they declare no distress (demon� strated by lack of anxiety, obsessions, guilt, or shame) about these paraphilic impulses and are not impaired in other important areas of functioning because of this sexual interest, and their psychiatric or legal histories indicate that they do not act on it, they could be ascertained as having frotteuristic sexual interest but should not be diagnosed with frotteuristic disorder. Nondisclosing individuals include, for instance, individuals known to have been touching or rubbing against nonconsenting individuals on separate occasions but who contest any urges or fantasies concerning such sexual behavior. Such individuals may re� port that identified episodes of touching or rubbing against an unwilling individual were all unintentional and nonsexual. Others may disclose past episodes of touching or rubbing against nonconsenting individuals but contest any major or persistent sexual interest in this. Since these individuals deny having fantasies or impulses about touching or rubbing, they would consequently reject feeling distressed or psychosocially impaired by such impulses. Despite their nondisclosing position, such individuals may be diagnosed with frotteuristic disorder. Recurrent frotteuristic behavior constitutes satisfactory support for frotteurism (by fulfilling Criterion A) and concurrently demonstrates that this paraphili cally motivated behavior is causing harm to others (by fulfilling Criterion B). Fewer victims can be intefireted as satisfying this criterion if there were multiple occasions of touching or rubbing against the same unwilling individ� ual, or corroborating evidence of a strong or preferential interest in touching or rubbing against nonconsenting individuals. Note that multiple victims are a sufficient but not a nec� essary condition for diagnosis; criteria may also be met if the individual acknowledges in� tense frotteuristic sexual interest with clinically significant distress and/or impairment. The Criterion A time frame, indicating that signs or symptoms of frotteurism must persist for at least 6 months, should also be intefireted as a general guideline, not a strict threshold, to ensure that the sexual interest in touching or rubbing against a nonconsenting individual is not transient. Hence, the duration part of Criterion A may also be met if there is clear evidence of recurrent behaviors or distress over a shorter but nontransient time period. Prevaience Frotteuristic acts, including the uninvited sexual touching of or rubbing against another individual, may occur in up to 30% of adult males in the general population. Approximately 10%-14% of adult males seen in outpatient settings for paraphilic disorders and hypersex� uality have a presentation that meets diagnostic criteria for frotteuristic disorder. Hence, whereas the population prevalence of frotteuristic disorder is unknown, it is not likely that it exceeds the rate found in selected clinical settings. Development and Course Adult males with frotteuristic disorder often report first becoming aware of their sexual in� terest in surreptitiously touching unsuspecting persons during late adolescence or emerging adulthood. However, children and adolescents may also touch or rub against unwilling oth� ers in the absence of a diagnosis of frotteuristic disorder. Although there is no minimum age for the diagnosis, frotteuristic disorder can be difficult to differentiate from conduct-disor� dered behavior without sexual motivation in individuals at younger ages. Frotteuristic disorder, however, by definition requires one or more contributing factors that may change over time with or without treatment: subjec� tive distress. As with other sexual preferences, advanc� ing age may be associated with decreasing frotteuristic sexual preferences and behavior. Nonsexual antisocial behavior and sexual preoccupation/hypersexuality might be nonspecific risk factors, although the causal relationship to frotteurism is uncertain and the specificity unclear. However, frotteurism is a necessary precondition for frotteuristic disorder, so risk factors for frotteurism should also increase the rate of frotteuristic disorder. G ender-Related Diagnostic Issues There appear to be substantially fewer females with frotteuristic sexual preferences than males. Conduct disorder in adolescents and antisocial personality disorder would be characterized by additional norm-breaking and antisocial behaviors, and the specific sexual interest in touching or rubbing against a nonconsenting individual should be lacking. Substance use disorders, particularly those involving stimu� lants such as cocaine and amphetamines, might involve single frotteuristic episodes by in� toxicated individuals but should not involve the typical sustained sexual interest in touching or rubbing against unsuspecting persons. Hence, recurrent frotteuristic sexual fantasies, urges, or behaviors that occur also when the individual is not intoxicated sug� gest that frotteuristic disorder might be present. Comorbidity Known comorbidities in frotteuristic disorder are largely based on research with males suspected of or convicted for criminal acts involving sexually motivated touching of or rubbing against a nonconsenting individual. Hence, these comorbidities might not apply to other individuals with a diagnosis of frotteuristic disorder based on subjective distress over their sexual interest. Conditions that occur comorbidly with frotteuristic disorder in� clude hypersexuality and other paraphilic disorders, particularly exhibitionistic disorder and voyeuristic disorder. Conduct disorder, antisocial personality disorder, depressive disorders, bipolar disorders, anxiety disorders, and substance use disorders also co-occur. Potential differential diagnoses for frotteuristic disorder sometimes occur also as comor bid disorders. Therefore, it is generally necessary to evaluate the evidence for frotteuristic disorder and possible comorbid conditions as separate questions. Over a period of at least 6 months, recurrent and intense sexual arousal from the act of being humiliated, beaten, bound, or othenwise made to suffer, as manifested by fan� tasies, urges, or behaviors. The fantasies, sexual urges, or behaviors cause clinically significant distress or impair� ment in social, occupational, or other important areas of functioning. Specify if: With asphyxiophilia: If the individual engages in the practice of achieving sexual arousal related to restriction of breathing. Specify if: In a controlled environment: this specifier is primarily applicable to individuals living in institutional or other settings where opportunities to engage in masochistic sexual behaviors are restricted. In full remission: There has been no distress or impairment in social, occupational, or other areas of functioning for at last 5 years while in an uncontrolled environment.
Radiation from the seeds travels a very short distance buy generic azelex 15g line, so the seeds can give off a large amount of radiation in a very small area discount azelex 15g fast delivery. Usually buy generic azelex 15g on line, around 100 seeds are placed cheap 15g azelex with amex, but this depends on the size of the prostate. Because the seeds are so small, they seldom cause discomfort, and are simply left in place after their radioactive material is used up. You may also get external beam radiation along with brachytherapy, especially if there is a higher risk that your cancer has spread outside the prostate (for example, if you 11 have a higher Gleason score). Hollow needles are placed through the skin between the scrotum and anus and into the prostate. Radioactive iridium-192 or cesium 137 is then placed in the catheters, usually for 5 to 15 minutes. Generally, about 1 to 4 brief treatments are given over 2 days, and the radioactive substance is removed each time. For about a week after treatment, you may have some pain or swelling in the area between your scrotum and rectum, and your urine may be reddish-brown. Possible risks and side effects of brachytherapy 21 American Cancer Society cancer. Even though the radiation doesn�t travel far, your doctor may advise you to stay away from pregnant women and small children during this time. If you plan on traveling, you might want to get a doctor�s note regarding your treatment, as low levels of radiation can sometimes be picked up by detection systems at airports. You may be asked to strain your urine for the first week or so to catch any seeds that might come out. You may be asked to take other precautions as well, such as wearing a condom during sex. There have also been reports of the seeds moving through the bloodstream to other parts of the body, such as the lungs. As far as doctors can tell, this is uncommon and doesn�t seem to cause any ill effects. Bowel problems: Brachytherapy can sometimes irritate the rectum and cause a condition called radiation proctitis. Bowel problems such as rectal pain, burning, and/or diarrhea (sometimes with bleeding) can occur, but serious long-term problems are uncommon. Urinary problems: Severe urinary incontinence (trouble controlling urine) is not a common side effect. But some men have problems with frequent urination or other symptoms due to irritation of the urethra, the tube that drains urine from the bladder. Rarely, the urethra may actually close off (known as a urethral stricture) and need to be opened with a catheter or surgery. Erection problems: Some studies have found rates of erection problems to be lower after brachytherapy, but other studies have found that the rates were no different than with external beam radiation or surgery. The younger you are and the better your sexual function before treatment, the more likely you will be to regain function after treatment. Erection problems can often be helped by treatments such as those listed in the surgery section, including medicines. For more about coping with erection problems and 12 other sexuality issues, see Sexuality for the Man With Cancer. Stereotactic body radiation therapy versus intensity modulated radiation therapy for prostate cancer: Comparison of toxicity. Five-year outcomes after prostatectomy or radiotherapy for prostate cancer: the Prostate Cancer Outcomes Study. Rectum-spacer related acute toxicity endoscopy results of 403 prostate cancer patients after implantation of gel or balloon spacers. Last Medical Review: August 1, 2019 Last Revised: August 1, 2019 Cryotherapy for Prostate Cancer Cryotherapy (also called cryosurgery or cryoablation) is the use of very cold temperatures to freeze and kill prostate cancer cells as well as most of the prostate. Even though it is sometimes being called cryosurgery, it is not actually a type of surgery. Cryotherapy is sometimes used if the cancer has come back after radiation therapy. It may be an option to treat men with low risk early-stage prostate cancer who cannot have surgery or radiation therapy. However, most doctors do not use cryotherapy as the first treatment for prostate cancer. This type of procedure requires spinal or epidural anesthesia (the lower half of your body is numbed) or general anesthesia (you are asleep). Very cold gases are then passed through the needles to freeze and destroy the prostate. To be sure the prostate is destroyed without too much damage to nearby tissues, the doctor carefully watches the ultrasound during the procedure. Warm saltwater is passed through a catheter in the urethra during the procedure to keep it from freezing. After the procedure, you might need to stay in the hospital overnight, but many men go home the same day. Cryotherapy is less invasive than surgery, so there is usually less blood loss, a shorter hospital stay, shorter recovery period, and less pain. But compared with surgery or radiation therapy, doctors know much less about the long-term effectiveness of cryotherapy. And as with brachytherapy, this may not be a good option for men with large prostate glands. Possible side effects of cryotherapy Side effects from cryotherapy tend to be worse if it is done in men who have already had radiation therapy, compared to men who have it as the first form of treatment.
Cheap azelex 15g with amex. Vigore वियाग्रा ke SIDE Effects kya hai ? Dose ? Over Dose ? Precautions ? #MedKYC.