
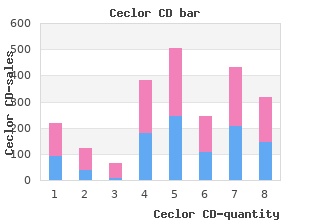
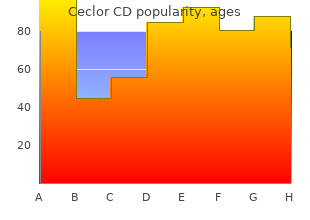
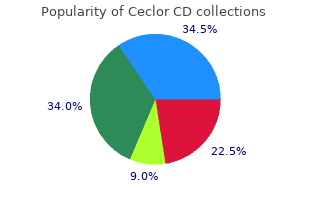
Ceclor CD
"375mg ceclor cd with mastercard, prophylactic antibiotics for uti guidelines."
By: William A. Weiss, MD, PhD
- Professor, Neurology UCSF Weill Institute for Neurosciences, University of California, San Francisco, San Francisco, CA

https://profiles.ucsf.edu/william.weiss
Three such procedures are currently being evaluated as part of research protocols: G in utero closure of spina bifida during the second trimester of pregnancy by performing a maternal hysterotomy order 375mg ceclor cd otc antimicrobial q tips. Initial animal studies suggested that early closure protected the exposed spinal cord from trauma and the neurotoxic effects of amniotic fluid and improved neurological function cheap ceclor cd 375mg overnight delivery antibiotic used for bronchitis. These observations have yet to be replicated in the human25 G endoscopic placement of a balloon inflated in the fetal trachea to improve lung growth and improve outcome with congenital diaphragmatic hernia22 G percutaneous vesicoamniotic shunting in male fetuses with presumed posterior urethral valves effective 375 mg ceclor cd antibiotic resistance farming. Conclusions G Technical improvements in ultrasound equipment continue to be made – more recently generic ceclor cd 375mg free shipping antibiotic list, 3- D ultrasound technology has been introduced for diagnostic purposes, although its exact role remains unclear. G Experience from fetal diagnosis is leading to a better understanding of the natural history of many fetal disorders which previously were derived principally from postnatal obser- vations. G While amniocentesis, chorionic villus sampling and fetal blood sampling remain standard methods for the diagnosis of aneuploidy, noninvasive techniques are being developed which should reduce the need for invasive procedures in the future. G In utero treatment of some structural abnormalities has been practised for a number of years but it is recognised that such interventions need to be tested in well-designed prospective studies to establish their effectiveness. Management following a diagnosis of a fetal abnormality Current national guidelines recommend that routine screening for trisomy 21 should be performed before 14 completed weeks of pregnancy to allow early decisions to be made, including whether to have an invasive diagnostic test and, if fetal aneuploidy is confirmed, whether to have the pregnancy terminated. Information for women about antenatal screening Screening for trisomy 21 and fetal anomalies is universally offered to women, who must be provided with accurate information and the opportunity to discuss the purpose and potential outcomes of all antenatal screening tests so that they may decide whether to accept or decline the tests. The provision of information and pre-test discussions should be scheduled early enough to enable a woman to have time to decide whether to have screening. Nationally produced written information on antenatal screening is available and has been translated into several languages. Fetal anomaly screening using ultrasound scanning at 18+0 days to 20+6 weeks is offered to all women. Even when women are well- informed about the purpose of tests including scans, the emotional impact of a diagnosis of abnormality is highly significant and causes considerable distress. The shock of any prenatal diagnosis of fetal abnormality makes it hard for women to take in the information that they need to assimilate to make potentially life-changing decisions. It is essential, therefore, when a diagnosis is made, to have well-planned and well-coordinated care pathways in place in all units. Communication of findings from chorionic villus sampling and amniocentesis Some women will undergo invasive diagnostic procedures for chromosomal or genetic abnor- malities following an abnormal fetal anomaly screening test or because of family history. Whatever the reason, a positive test result will lead to difficult decisions about the future of the pregnancy. How and when the results will be delivered should be agreed before the test is performed and the professional responsible should be suitably trained to discuss difficult infor- mation with patients. Following the diagnosis of a chromosomal abnormality, the woman concerned should be 21 offered a consultation with her obstetrician as soon as possible to discuss the results and her options. Better implementation of screening tests is likely to result in an increase in first- trimester diagnoses of aneuploidy and other abnormalities, which will lead to more women being offered an earlier surgical termination of pregnancy. There is, however, no evidence that earlier termination of pregnancy lessens the emotional impact of the pregnancy loss. Communication of findings from ultrasound Regardless of how a fetal abnormality is detected, it is essential that there is a clearly defined care pathway to ensure that appropriate information and support are available. Figure 2 shows the screening pathway for a woman with a scan with suspected fetal anomaly detected at 18– 20 weeks. Abnormality identified or suspected Second sonographer Local protocol may permit direct referral with severe abnormality (anencephaly) Confirmed or suspected No abnormality found Second opinion Obstetrician required Obstetric ultrasound specialist (fetal medicine specialist or radiologist If feticide required Fetal medicine Confirmed unit Confirmed Feticide Terminate Continue with pregnancy Abnormality Primary care team not confirmed Figure 2 Screening pathways for ultrasound diagnosis If the scan reveals either a suspected or confirmed abnormality, the woman should be informed 22 by the sonographer at the time of the scan. It is essential that all practitioners performing fetal anomaly ultrasound screening should be trained to communicate abnormal findings to women, as such information is likely to have significant emotional impact. Usually, sonographers will ask a senior sonographer colleague to confirm findings and this should be done immediately. If an abnormality is confirmed or suspected, referral is usually required, although some obvious major fetal abnormalities, such as anencephaly, may not require a second opinion (this should be decided by local guidelines). For women who have been given distressing news about their baby during the scan, there should be a health professional available to provide immediate support. In the case of a suspected abnormality, women should be seen for a second opinion by an expert in fetal ultrasound, such as a fetal medicine specialist. An appointment should be arranged as soon as possible and ideally within three working days. Any delay in receiving more information about the abnormality and its implications will be distressing for women and this should be acknowledged. If the specialist cannot confirm the abnormality and is confident that the fetus is developing normally, the woman should still be referred to her obstetrician for further discussion, because the significance, from the woman’s perspective, of a temporary ‘false positive’ and the associated residual anxiety should not be underestimated and support and explanation will be required. Once an abnormality has been confirmed, arrangements should be made for the woman to see an expert who has knowledge about the prognosis of the abnormality and the options available. For most abnormalities, this will be a fetal medicine expert, although some women may want to discuss their decision further with their local obstetrician. When an offer of termination is deemed appropriate the decision to end what is usually a wanted pregnancy is extremely difficult and painful for most parents. Women and their partners will need as much information as possible on the implications of the diagnosis. Obstetricians are not always best placed to advise on outcomes after birth and, in some situations, input from other medical specialists, such as paediatricians, paediatric surgeons, geneticists and neonatologists, may be required to ensure a more comprehensive and balanced approach. Agreement on the diagnosis and as precise a prognosis as possible provides the woman with the best available information on which to make her decision when she is counselled by the fetal medicine specialist or subspecialist. Counselling and support the decision-making process for women and their partners after the diagnosis of fetal abnor- mality is a difficult one. They must try to absorb the medical information they have been given, while in a state of emotional shock and distress, and work out a way forward that they can best live with. In such sensitive circumstances, women and their partners must receive appro- priate counselling and support from the healthcare practitioners involved. All staff involved in the care of a woman or couple facing a possible termination of pregnancy must adopt a non- directive, non-judgemental and supportive approach.
Evaluation and treatment of menorrhagia treatment should be made after taking into account the in an adolescent population effective 375 mg ceclor cd antibiotic resistance hsc. Menstruation among decreases the quality of life and is worrisome for both the adolescent girls in Malaysia: a cross-sectional school survey ceclor cd 375mg without a prescription liquid oral antibiotics for acne. Study Group on Menstrual evaluations to determine the cause should be completed ceclor cd 375mg lowest price infection low temperature, Disorders discount ceclor cd 375 mg without prescription virus living. London: Royal College of Obstetricians and treatments that will rapidly restore haemodynamic stabil- Gynecologist; 2000:141-52. Dysfunctional uterine bleeding ity should be administered via an algorithm for patients during adolescence. Menstrual disorders and abnormal school performance and on the social activities of this genital tract bleeding. Thessaloniki: University Studio Press; episodes without damaging the hormonal axis during the 2004:419-50. Prostaglandin Conflict of Interests synthesis in the endometrium of women with ovular the authors declare no conflicts of interests. Bleeding disorders in teenagers presenting with patterns in the early postmenarcheal period, duration of menorrhagia. Management of heavy menstrual only medical therapy for outpatient management of bleeding in adolescents. Screening for coagulation of menorrhagia in women with inherited bleeding disorders in adolescents with abnormal uterine bleeding. Copyright © 2017 the Author (s); This is an open-access article distributed under the terms of the Creative Commons Attribution License creativecommons. Betensky aElectrophysiology Program, Cardiovascular Division, Department of Medicine, Hospital of the University of Pennsylvania, Philadelphia, Pennsylvania, United States bUnidad de Electrofisiologıa´ Cardiaca, Servicio de Cardiologıa,´ Hospital de Basurto, Bilbao, Vizcaya, Spain Article history: A B S T R A C T Available online 21 December 2011 Cardiac arrhythmias are prevalent among humans across all age ranges and may occur in the setting of Keywords: underlyingheart diseaseas well as instructurallynormal hearts. Whilearrhythmias arewidely variedin Automaticity their clinical presentations, they possess shared electrophysiologic properties at the cellular level. Reentry Although identifying the specific mechanism may at times be challenging for the clinician and require invasive electrophysiologic study, differentiating and understanding the underlying mechanismmay be critical to the development of an appropriate diagnosis and treatment strategy. Mecanismos de las arritmias cardiacas R E S U M E N Palabras clave: En la especie humana, las arritmias cardiacas son muyprevalentes entodos los grupos de edad y pueden Automatismo darse tanto en el contexto de una cardiopatıa´ subyacente como en corazones estructuralmente Actividad desencadenada normales. Aunque las formas de presentacion´ clınica´ de las arritmias son muy diversas, en las celulas´ Reentrada comparten propiedades electrofisiologicas´ comunes. Los 3 mecanismos principales de las arritmias cardiacas son las alteraciones en el automatismo, la actividad desencadenada y la reentrada. Aunque la identificacion´ del mecanismoespecıfico´ avecespuedaresultardifıcil´ paraelclınico´ yrequerirunestudio electrofisiologico´ invasivo, diferenciar y comprender el mecanismo subyacente puede ser crucial para desarrollar una correcta estrategia diagnostica´ y terapeutica. When it reaches À40 mV, calcium (Ca2+) bothconductionof electrical impulsesandmechanicalcontraction. Subsequently, outward potassium (K+) depolarization and to initiate an electrical impulse in the absence currents are activated and Ca2+ currents are inactivated. Upon reaching the resting gated through cardiac myocytes, which are excitable, referring to membrane potential, the cycle is ready to repeat itself. At this point, Na+ channels are triggered to open, * Corresponding author: Hospital of the University of Pennsylvania, 9th Floor, resulting in a large but transient inward Na+current (phase 0). The Founders Pavilion, 3400 Spruce Street, Philadelphia, Pennsylvania 19104, United States. Na+ current is quickly inactivated, followed by a subsequent outward K+current and thereby initiating repolarization (phase 1). The I is the main route for Ca2+ influx Ca,L and triggers Ca2+ release from the sarcoplasmic reticulum, initiating contraction of the myocyte. Activation of delayed rectifier K+ channels and inactivation of Ca2+ channels leads to termination of the plateau and initiates late repolarization (phase Absolute Relative 3). Finally, outward K+ channels mediate the final repolarization refractoriness refractoriness (phase 4). Refractory periods, showing the absolute and relative refractory periods during the action potential. The refractory period is defined by the time interval following excitation during which the cell remains unexcitable. Table 1 This is due to the lack of availability of depolarizing current (which Mechanisms of Cardiac Arrhythmias is Na+ in muscle cells). It is classified as either absolute or relative Disorders of impulse formation Disorders of impulse (Fig. Purkinje system, as well as some cells in both atria,5 possess the Parasympathetic activity reduces the discharge rate of the property of pacemaker activity or automaticity. The suppressive effect of Ach is frequently used in practice for the firing rate is determined by the interaction of 3 factors: the both diagnostic and therapeutic purposes. Catecholamines increase the permeability of Ica-L, increasing the inward Ca2+ current. Sympathetic activity also results in enhance- −40 −40 3 ment of the I current,8 thereby increasing the slope of phase 0 f 4 repolarization. Metabolic abnormalities such as hypoxia and hypokalemia can −80 −80 4 lead to enhanced normal automatic activity as a result of Na/K pump inhibition, thereby reducing the background repolarizing current and enhancing phase 4 diastolic repolarization. B:muscle In degenerative conditions that affect the cardiac conduction cell action potential. D: increased numerous currents that together result in a net inward depolariz- slopephase4depolarization. The intrinsic rate of an automatic abnormal focus depends on the membrane potential; the more positive the membrane potential, the faster the automatic rate. A subsidiary is thought to play a role in cases of elevated extracellular pacemaker may manifest as a result of suppression of sinus potassium, low intracellular pH, and catecholamine excess. An important distinction between enhanced normal and the hallmark of normal automaticity is ‘‘overdrive suppres- abnormal induced automaticity is that the latter is less sensitive sion.
The information gathered is the foundation of the evidence to determine if a technology is effective and safe for use in a particular clinical population or setting purchase ceclor cd 375mg online virus 68 symptoms 2014. Information is collected to understand how a new technology fits within current practice and treatment alternatives order ceclor cd 375 mg bacteria names a-z. Details of the technology’s diffusion into current practice and information from practicing medical experts and industry generic 375 mg ceclor cd free shipping tick treatment for dogs frontline, adds important information to the review of the provision and delivery of the health technology in Ontario cheap ceclor cd 375 mg mastercard virus not alive. Information concerning the health benefits; economic and human resources; and ethical, regulatory, social and legal issues relating to the technology assist policy makers to make timely and relevant decisions to maximize patient outcomes. The public consultation process is also available to individuals wishing to comment on an analysis prior to publication. It also incorporates, when available, Ontario data, and information provided by experts and applicants to the Medical Advisory Secretariat to inform the analysis. While every effort has been made to do so, this document may not fully reflect all scientific research available. Additionally, other relevant scientific findings may have been reported since completion of the review. Please check the Medical Advisory Secretariat Website for a list of all evidence-based analyses:. Clinical Need Atrial fibrillation is characterized by an irregular, usually rapid, heart rate that limits the ability of the atria to pump blood effectively to the ventricles. Atrial fibrillation can be a primary diagnosis or it may be associated with other diseases, such as high blood pressure, abnormal heart muscle function, chronic lung diseases, and coronary heart disease. Symptoms caused by decreased blood flow include dizziness, fatigue, and shortness of breath. The drug selection process frequently involves trial and error until the patient’s symptoms subside. For instance, radiofrequency energy uses heat to burn tissue near the source of the arrhythmia. The purpose is to create a series of scar tissue, so that the aberrant electrical pathways can no longer exist. There are 2 methods of ablation: catheter ablation and surgical (operative) ablation. Catheter ablation involves inserting a catheter through the femoral vein to access the heart and burn abnormal foci of electrical activity by direct contact or by isolating them from the rest of the atrium. Ablation for Atrial Fibrillation - Ontario Health Technology Assessment Series 2006; Vol. The Medical Advisory Secretariat also searched Medscape on the Internet for recent reports on trials that were unpublished but that were presented at international conferences. Search terms included: radiofrequency ablation, catheter ablation and atrial fibrillation. First-line Catheter Ablation for Atrial Fibrillation or Atrial Flutter Both studies concluded that catheter ablation was associated with significantly improved long-term freedom from arrhythmias and quality of life compared with medical therapy. Catheter ablation as first-line treatment is considered experimental at this time. Ablation technology is continually evolving with increasing success rates associated with the ablation procedure. Ablation for Atrial Fibrillation - Ontario Health Technology Assessment Series 2006; Vol. Background Clinical Need: Target Population and Condition Atrial fibrillation is a highly prevalent chronic condition. Normal Heart Rhythm (Sinus Rhythm) In a normal heart, the electrical pathway flows from the right atrium to the left atrium, which causes the muscles of the atria to contract and allows blood to be pumped from the atria to the ventricles. Arrhythmias occur when there is a problem with the flow of electrical current through the heart. Atrial Fibrillation Atrial fibrillation is characterized by an irregular, usually rapid, heart rate. He demonstrated through a computer model that interlacing waves of activity could sustain arrhythmia. The ventricles are unable to fill to their full capacity between contractions, which means that blood is ineffectively being pumped through the body. Atrial fibrillation may spontaneously revert to sinus rhythm, or a patient may require an intervention (such as electrical cardioversion) to convert back to sinus rhythm. Ablation for Atrial Fibrillation - Ontario Health Technology Assessment Series 2006; Vol. Symptoms caused by decreased blood flow include dizziness, fatigue, and shortness of breath. The rapid contractions or quivering of the atria can cause blood to stagnate inside the atria with the formation of blood clots, which, if dislodged, can cause strokes. Table 1 provides the prevalence by age and gender (derived from results of Go et al. Table 1: Prevalence of Atrial Fibrillation in Ontario (People Aged Over 20 Years)*† Male Pop. The rapid yet regular heart rhythm is due to a constant reentrant system in the right atrium. Usually re-entry occurs in a counterclockwise motion up the atrial septum and the down the lateral wall of the right atrium. Reciprocating Tachycardias Reciprocating tachycardias involve the accessory pathways. Accessory pathways refer to abnormal muscular connections between the atria and ventricles. Atrial Tachycardia Atrial tachycardia is characterized by a rapid, regular atrium rhythm usually due to intra-atrial re-entry or an ectopic atrial focus. There are various causes of atrial tachycardia including atrial irritation due to pericarditis, inflammation of the pericardium, the fibrous sac that surrounds the heart; and drug or chemical toxicity.
This study has suggested that the lat- highestincidenceofonsetinthe1styearoflifefollowed eral femoral cutaneous nerve is most prone to damage by a second peak between the ages of 16 and 20 order ceclor cd 375mg visa bacteria que se come la carne. It may al- course of the genitofemoral generic 375 mg ceclor cd fast delivery virus back pain, lateral femoral buy 375 mg ceclor cd amex antibiotics for uti during pregnancy, and ilioin- 24 1 Anatomy of the Abdominal Wall guinal nerves and their relationships to the deep ingui- Surgical relief may require a superolateral cut to avoid nal ring buy cheap ceclor cd 375mg online treatment for uncomplicated uti, iliopubic tract, and anterior superior iliac any possible injury to the inferior epigastric vessels. The findings indicate It may appear in infancy or early adult life subse- that both branches of the genitofemoral nerve pene- quent to forced opening of a preexisting or partially tratetheabdominalwalllateraltothedeepinguinal patent processus vaginalis during a strenuous activity, ring and cranial to the iliopubic tract. The ilioinguinal such as lifting of heavy objects, or repeated stresses on and lateral femoral cutaneous nerves pursued a course the wall during sneezing, coughing or vomiting. Inthefe- mately 10% of the pelves examined the lateral femoral male, the hernial sac descends through a much narrow- cutaneous nerve was found either within a half-centi- er canal to the major labium; as a result, palpation of the meter of the iliopubic tract or in the vertical plane of hernial sac is not adequate. These are the principal with women in whom the expanding impulse on cough- anchoring sites for mesh in laparascopic hernial repair. In another study, the lateral femoral cutaneous nerve wasmostcommonlyfoundat10–15mmfromthean- 1. Direct inguinal hernia is a form of acquired outpouch- ing in which the hernial sac runs through the posterior wall of the inguinal canal and protrudes through the 1. The su- cavity of the abdomen and that of the scrotum or major pravesical fossa [57–59] lies superior to the urinary labium. Indirect inguinal hernia is common in all ages bladder between the medial and median umbilical liga- andinbothsexes. Since the conjoint tendon is anterior to the su- that patent processus vaginalis is not always a prerequi- pravesical fossa and posterior to the superficial ingui- site for the occurrence of indirect inguinal hernia. It is nal ring, the hernial sac either passes between the fi- often associated with cryptorchid testis and hydrocele. When the hernial sac pierces the conjoint complication of spilled gallstones [54–56]. Persistent tendon it will be covered by the peritoneum as well as processus vaginalis may be unmasked by the presence by the aponeurosis of the internal abdominal oblique of fluid that fills this peritoneal extension and presents and transverse abdominis muscle. In a large Hesselbach’s triangle is bounded medially by the indirect inguinal hernia, the inguinal canal is no longer rectus abdominis, laterally by the inferior epigastric oblique due to the close proximity of the dilated super- vessels, and inferiorly by the inguinal ligament [60]. Since the deep inguinal When the hernial sac passes through Hesselbach’s tri- ring lies lateral to the inferior epigastric vessels, the angle, it is usually lateral to the conjoint tendon and neck of the hernial sac protrudes through the lateral in- will be invested by the extraperitoneal fat, transversalis guinal fossa, shifting these vessels medially. As it tra- fascia, external spermatic fascia, superficial fascia, and verses the deep inguinal ring, the hernial sac is invested the skin. After pushing up the spermatic cord is usually posterolateral to the hernial arching fibers of the transverse and internal abdominal sac, not posterior to it as in indirect hernia. When the oblique, it becomes invested by the cremasteric muscle hernial sac is occasionally large, it may protrude into and fascia. Since the path of the hernial sac does not blood supply compromised at the deep inguinal ring. On standing, the hernial sac is felt as a dif- dence is far lower than that of inguinal hernia and can fuse medial outpouching over the inguinal canal, which be easily missed during physical examination. It is dence of femoral hernia postinguinal herniorrhaphy an acquired condition associated with obesity, consti- compared with spontaneous incidence. It is usually ity of the femoral hernia in children and the similarity asymptomatic and is even less noticeable than the indi- of its manifestations to that of the indirect inguinal her- rect type. This type of hernia is not contained in the nia, femoral hernia in this population remains a chal- spermatic cord, and unless the hernial sac is large it lenging clinical problem. The her- Misdiagnosis of femoral hernia may be perpetuated nial sac protrudes anteriorly and pushes the side of the bythepresenceofapatentprocessusvaginalisandin- examiner’s index finger forward. A variety of rect inguinal hernia may protrude on each side of the conditions must be excluded in the differential diagno- inferior epigastric vessels as pantaloon hernia. Itfrequentlycon- anterior to the pectineal (Cooper’s) ligament and tains the small intestine and omentum, but the pres- throughthefemoralcanal,apotentialspacebetween ence of an inflamed appendix, Meckel’s diverticulum, the lacunar ligament and the femoral vein. Oc- ring, which is the upper margin of the femoral canal, is casionally the ureter or broad ligament of the uterus the medial portion of the lacuna vasorum. Femoral hernial sac becomes irre- ed anteriorly by the extension of the transversalis fas- duciblewhenitattainsalargesize,protrudinganterior cia, and posteriorly by the continuation of the pectineal to the inguinal ligament. The neck of the hernial sac is always distal and boundaries, the hernial sac carries a higher risk of lateral to the pubic tubercle, a bony landmark between strangulation and should be considered part of the dif- the site of inguinal and femoral hernia. The fundus of ferential diagnosis in pregnant women and in individu- the hernial sac (lower part) usually occupies the medial als with intestinal obstruction. The hernial sac may turn medially Umbilical hernia, common among African-American and toward the scrotum or major labium. It may also children, is associated with failure of complete closure descend anterior (prevascular hernia) or posterior of the umbilical orifice during the 1st year of postnatal (retrovascular hernia) to the femoral vessels. It is often noticed when the infant cries, which vented from descending further down by the attach- raises the intra-abdominal pressure and causes protru- ment of the femoral sheath and the superficial fascia of sion of part of the intestine. The when the defect is relatively large and persists beyond course of progression of the hernial sac should be taken the age of 4, or becomes incarcerated. In the adult, um- into consideration and reduction of femoral hernia bilical hernia may develop more commonly in women, should be directed in the reverse direction with the usually postpartum, and a pose serious danger due to thighs passively flexed. It affects approximately 35% of the fe- Herniation immediately above or below the umbilicus male population particularly in women over 50 years of is known as paraumbilical hernia, and occurs in women age. It is usually prone to incarcer- uniqueshapeofthepelvis,thesizeofthering,andthe ation and usually contains part of the greater omentum. It is classified as congenital and through the umbilical ring into the base of the umbili- acquired; the acquired lumbar hernia is subdivided in- cal cord.
The cited papers are selected and summarized due to perceived relevance and quality generic ceclor cd 375mg antibiotics for sinus infection and bronchitis, and in the interest of keeping it short cheap ceclor cd 375 mg with amex bacteria 100x. However purchase ceclor cd 375mg amex antibiotics have no effect on quizlet, many of these patients were symptomatic on beforehand generic ceclor cd 375 mg otc antibiotics not working for strep, and many were children. It is well known that the risk of an event is highest early in life and higher among subjects who have already had one or more events. According to the review paper cited above (1), the lifetime risk of (aborted) sudden death is approx. The risk of (aborted) cardiac arrest is lower if the subject has survived, symptom free, to the age of 40, according to a paper specifically addressing this (4). Recommendations: Even though the literature is very detailed, the recommendations have to be practical, if the rules are going to be adhered to. Young patients with the condition should be advised not to start a professional driving career, due to the consequences of a later syncope. All subjects must be aware of medications and circumstances that could provoke an arrhythmia. There are several variants, of which the so called type 1 is the only one with accepted clinical relevance. The prevalence (of type 1) is probably about 0,02% in Europe and 0,1% worldwide (1). Persons with Brugada syndrome should avoid certain drugs (with sodium channel blocking properties) (2). As the syndrome carries a risk of syncope and sudden, arrhythmic death, it may be relevant to driving. However, there is a tendency that these events occur during sleep or other vagal activity. Based on studies with a total of 1545 patients, the overall event rate was 10% over 2,5 years. Annual event rates are not given for the subgroups, but from the relative risks given and the overall event rate, the event rates seem to be in reasonable agreement with the ones given in (3), especially since syncope was included in (4) but not (3). Giustetto C et al: Risk stratification of the patients with Brugada type electrocardiogram: a community-based prospective study. Other cardiomyopathies the risk of sudden incapacitating events shall be evaluated in applicants or drivers with well described cardiomyopathies (e. Cardiovascular conditions or diseases can lead to a sudden impairment of the cerebral functions that constitutes a danger to road safety. These conditions represent grounds for establishing temporary or permanent restrictions to driving. When more than one disease coexists, the more restrictive recommendation prevails. All cardiovascular diseases in this section carry the risk of progression, and therefore in all cases the issue or renewal of the licence may be subject to periodic assessment especially if there is risk of deterioration. Brady-arrhythmias: sinus node disease and conduction disturbances Group 1: Driving licences will not be issued to, or renewed for, applicants or drivers with a history of syncope or syncopal episodes due to arrhythmic conditions. Driving licences may be issued, or renewed, after the condition has been effectively treated and subject to competent medical authorization. Group 2: Driving licences will not be issued to, or renewed for, applicants or drivers with a history of syncope or syncopal episodes due to arrhythmic conditions. Driving licences may be issued to, or renewed, after the condition has been effectively treated and subject to competent medical authorization. Tachy-arrhythmias: supraventricular and ventricular arrhythmias Group 1: Driving licences will not be issued to, or renewed for, applicants or drivers with a history of syncope or syncopal episodes due to arrhythmic conditions. Driving licences may be issued, or renewed, after the condition has been effectively treated and subject to competent medical authorization. Group 2: Driving licences will not be issued to, or renewed for, applicants or drivers with a history of syncope or syncopal episodes due to arrhythmic conditions. Driving licences may be issued to, or renewed, after the condition has been effectively treated and subject to competent medical authorization. Permanent pacemakers Group 1: Driving licences may be issued to, or renewed for, applicants or drivers after pacemaker implantation or replacement. Adequate pacemaker function and satisfactory wound healing is to be confirmed by a competent medical authority. Group 2: Driving licences may be issued to, or renewed for, applicants or drivers two weeks after pacemaker implantation or replacement. Adequate pacemaker function and satisfactory wound 55 healing is to be confirmed by a competent medical authority. Automatic defibrillators Group 1: Driving licences may be issued to, or renewed for, applicants or drivers after defibrillator implantation or replacement. When the defibrillator is implanted for secondary prevention, a minimum period of three months of driving cessation is imposed. When the defibrillator is implanted for primary prevention a minimum period of two weeks of driving cessation is imposed. Adequate defibrillator function and sufficient wound healing is to be confirmed by a competent medical authority. After an appropriate defibrillator shock a minimum period of three months of driving cessation is imposed. After an inappropriate defibrillator shock driving cessation is imposed until measures to prevent subsequent inappropriate therapy are taken and confirmed by a competent medical authority. Group 2: Driving licences will not be issued to, or renewed for, applicants or drivers with a defibrillator.
Purchase 375mg ceclor cd otc. Mix Turmeric Coconut Oil And Ginger And Drink Before Sleeping - Results After The Night Are Amazing.