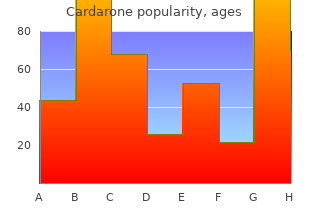

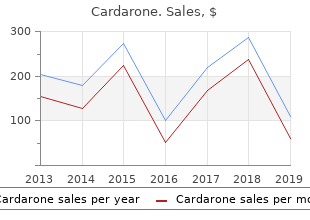
Cardarone
"Order 200 mg cardarone amex, heart disease 1 killer of women."
By: Bertram G. Katzung MD, PhD
- Professor Emeritus, Department of Cellular & Molecular Pharmacology, University of California, San Francisco
http://cmp.ucsf.edu/faculty/bertram-katzung
Select one of the following options: Rigid Twin Flexible Twin Coaxial Rigid Single 0 cheap cardarone 200mg otc blood vessels kids. The dielectric constant of the product is used for setting the appropriate signal amplitude thresholds generic cardarone 200mg fast delivery capillaries on face remove, see section Service and Troubleshooting for more information on amplitude threshold settings cheap cardarone 200mg cardiovascular systems inc. Normally cheap cardarone 200mg online arteries carry deoxygenated blood to the heart, this value does not need to be changed since the effect on measurement performance is very small for most vapors. Measurement Mode Model Measurement mode 3301 Level(1), Interface Immersed probe (1) 3302 Level, Level and Interface, Interface Immersed probe (1) Default setting. Interface Immersed Probe is used for applications where the probe is fully immersed in liquid. Note Only use Interface Immersed Probe for applications where interface is measured for a fully immersed probe. Do not change this value if the transmitter is mounted with the probe along the vertical line (which is normally the case). By setting this parameter, you can avoid that interface measurements get out of range. The Damping parameter determines how quickly the transmitter responds to level changes and how robust the measurement signal is against noise. If the 20 mA point is set to a point within the Transition Zone, the full range of the analog output is not used. If the 4 mA point is set to a point within the transition zone or below the probe end (tank bottom for example), the full range of the analog output is not used. See Transition zones on page 16 for more information on the size of upper and lower transition zones. Standard shapes are: Vertical Cylinder, Horizontal Cylinder, Vertical Bullet, Horizontal Bullet or Sphere. If your tank does not correspond to any of the above tank shapes, select Strap Table. See Volume configuration on page 64 for information on how to specify tank dimensions. The strapping points must be entered such that the first point corresponds to the lowest level, and the last point corresponds to the topmost level of the tank. You can select either of the following two methods to configure a Rosemount 3300 Series Transmitter: Start the Wizard for a guided installation if you are unfamiliar with the Rosemount 3300 Series. If communication is intermittent, increase Busy Retries and Error Retries to 5 and 5 respectively. If the F1 key is pressed, a help text appears with information about the window that is currently open. If a menu option is selected, a help text appears with information about that particular menu. Now you will be guided through a number of dialogs allowing you to configure the transmitter. This information is not required for the operation of the transmitter and can be left out if desired. Other variables like Product Distance, Interface Distance, Upper Product Thickness, etc. Set the Lower Range Value (4 mA) and the Upper Range Value (20 mA) to the desired values. Keep in mind that the 20 mA value must be below the upper transition zone, and the 4 mA point must be above the lower transition zone if you want to use the full 4-20 mA range within the measuring range of the transmitter. See Transition zones on page 16 for more information on upper and lower transition zones. See Basic configuration on page 69 for more information on setting the Upper and Lower Range values. The Damping parameter may be changed if there are high filling rates, see High level rates on page 98 for more information. The Rosemount 3300 Series Transmitter makes some initial calibrations automatically, based on the chosen probe type. The following probe types are available: Rigid twin Flexible twin Coaxial Rigid single 0. The probe length is the distance from the upper reference point to the end of the probe, see Figure 4-1 on page 62. The Reference Gauge Height is the distance from the upper reference point to the bottom of the tank (see Figure 4-1 on page 62). When setting the reference gauge height, keep in mind that this value is used for all level and volume measurements performed by the Rosemount 3300 Series Transmitter. The reference gauge height must be set in linear (level) units, such as feet or meters, regardless of primary variable assignment. Setup Environment the Environment tab contains information about measurement mode, the upper product dielectric constant and advanced environment options. Measurement Mode Model Measurement mode 3301 Level(1), interface immersed probe (1) 3302 Level, level and interface, interface immersed probe (1) Default setting. Interface immersed probe is used for applications where the probe is fully immersed in liquid. See Interface measurements with fully immersed probes on page 99 for more information. Note Use interface immersed Probe only for applications where interface is measured for a fully immersed probe. Dielectrics In some applications there is heavy vapor above the product surface having a significant influence on the level measurement. The default value is equal to 1, which corresponds to the dielectric constant of vacuum. For interface measurements, the dielectric constant of the upper product is essential for calculating interface level and the upper product thickness.
Furthermore cheap 200mg cardarone with mastercard blood vessels kidney, provocative discography has failed to buy 200mg cardarone with amex cardiovascular outpatient center alliance improve patient selection to buy cardarone 200mg visa coronary heart 1985 obtain better clinical outcome after surgery [177] generic cardarone 200mg fast delivery arteries veins and capillaries images. So far, facet joint injec must be made cautiously tions have been used for this purpose but are not without shortcomings (see Chapter 10). Some authors suggest that a facet joint syndrome can be diagnosed based on pain relief by an intra-articular anesthetic injection or provocation of the pain by hypertonic saline injection followed by subsequent pain relief after injection of local anesthetics [44, 173, 185, 199]. Interpretation of the pain response is difficult because the facet joints are innervated by two to three seg mental posterior branches and the local anesthetic may diffuse to adjacent levels if the injection is done non-selectively. We recommend using contrast injection to document the correct needle position and filling of the joint capsule (Case Study 1). Uncontrolled diag nostic facet joint blocks exhibit a false-positive rate of 38% and a positive predic tive value of only 31% [239]. It is therefore mandatory to perform repetitive in filtrations to improve the diagnostic accuracy [239]. However, there are no convincing pathognomonic, non-invasive radiographic, historical, or physical examination findings that allow the reliable identification of lumbar facet joints as a source of low-back pain and referred lower extremity pain [69, 70]. Temporary Stabilization Temporary stabilization the diagnosis of segmental instability remains a matter of intensive debate. How does not predict fusion ever, it would be unreasonable to assume that abnormal segmental mobility is outcome non-existent or cannot be painful. Imaging studies, particularly functional views, have failed to reliably predict segmental instability because of the wide normal range of motion. The temporary stabilization with a pantaloon cast [223] has the drawback of being unselective and requires further diagnostic testing. Stabilization of the putative abnormal segments by an external transpedicular fixator has been suggested by several authors [74, 237, 254] with mixed results in terms of outcome prediction. Based on an analysis of 103 cases, Bednar [10] could not support using the external spinal skeletal fixation as a pre dictor of pain relief after lumbar arthrodesis. So far, there is insufficient evidence to exclude patients from surgery on the grounds of specific risk factors [183]. Nonetheless, in the presence of selected fac tors (see Chapter 7), surgery should at least be delayed until attempts have been made to modify risk factors that are amenable to change and all possible conser vative means of treatment are exhausted. Degenerative Lumbar Spondylosis Chapter 20 553 Non-operative Treatment Most patients with predominant low-back pain without radiculopathy or claudi cation symptoms can be managed successfully by non-operative treatment modalities (Case Study 2). General objectives of treatment pain relief improvement of social activities improvement of health-related quality of life improvement of recreational activities improvement of activities of daily living improvement of work capacity When the diagnostic assessment has identified a specific source of back pain (Table 1), the conservative treatment option does not differ from those applied to non-specific disorders, which are extensively covered in Chapter 21. Themain stay of non-operative management rests on three pillars: pain management (medication) functional restoration (physical exercises) cognitive-behavioral therapy (psychological intervention) Pharmacologic pain management is outlined in Chapter 5. The first important aspect is a multidisciplinary to address fears and functional restoration program and psychological interventions to influence misbeliefs patient behavior (see Chapter 21). The longer pain and functional limitations persist, the less likely is pain relief, functional recovery and return to work (see Chapter 6). Patients presenting with specific degenerative back pain usually experience their pain and functional limitations for more than 3 months. These patients should promptly be included in a multidisciplinary functional work conditioning program. It is as simple as it is obvious that the outcome of any treatment is critically dependent on patient selection and this is also valid for non-operative treatment (see Chapter 7). The paradigm of spinal fusion is based on the experience that painful diarthrodial joints or joint deformities can be successfully treated by arthrodesis [66, 121]. Since its introduction in 1911 by Albee [3] and Hibbs [127], spinal fusion was initially only used to treat spinal infections and high-grade spondylolisthesis. Today approximately 75% of the interventions are done for painful degenerative disorders [66]. Despite its frequent use, spinal fusion for lumbar spondylosis is still not solidly based on scientific evidence in terms of its clinical effectiveness [66, 102, 103, 264]. For a long time it was hoped that outcome of spinal fusions could be significantly improved when the fusion rates come close to 100%. How ever, it is now apparently clear that outcome is not closely linked to the fusion sta tus [24, 90, 91, 102, 103, 256]. The standard concept advocated in the literature is that surgical treatment is indicated when an adequate trial of non-operative treatment has failed to improve the patient�s pain or functional limitations [122, 264]. However, there is no general consensus in the literature on what actually comprises an adequate trial of non-operative care. The gen eral philosophy that surgery is only indicated if long-term non-operative care has failed is challenged by the finding that the longer pain persists the less likely it is that it will disappear. This notion is supported by recent advances in our under standing of the pathways and molecular biology of persistent (chronic) pain (see Chapter 5). It has also been known for many years that returning to work becomes very unlikely after 2 years [268]. Surgery if needed should be Wethereforeadvocateamoreactive approach in patient selection for surgery, done in a timely manner i. This evaluation must be based on a thorough clini cal assessment, imaging studies and diagnostic tests. If a pathomorphological alter ation in concordance with the clinical symptoms can be found, the patient should be selected for potential surgery. Prior to surgery, the patient should then be inte grated in a fast track aggressive functional rehabilitation program (not longer than 3 months). If this program fails, the structural correlate should be treated surgically if multilevel (>2 levels) fusion can be avoided. In multilevel degeneration of the lumbar spine requiring more than two-level fusion, the clinical outcome is less sat isfactory in our hands and we are more conservative.
Usually the receiving team will designate a player to 200 mg cardarone fast delivery heart disease for kids be the handler before the pull 200 mg cardarone blood vessels that serve as gateways to capillary beds are, to discount cardarone 200mg fast delivery cardiovascular disease omega-3 fatty acids minimize confusion buy generic cardarone 200 mg on-line coronary heart 5k. If the disc hits the ground and begins rolling, any player on the receiving team can stop its progress without having to become the handler. If someone is counting too fast, you may call fast count; at this point they must go back 2 in the stall count. If they continue to count too fast and you call it again within the same stall count, the play stops and the count goes back to 0. Picks If any player on the field impedes the progress of a defensive player trying to check their offensive counterpart, the defensive player should call pick very loudly so play does not continue. The defensive player must be within 10 feet (3 meters) of their check to call a pick. A catching foul may be called when there is contact between opposing players in the process of attempting a catch, interception, or knock down. A certain amount of incidental contact during or immediately after the catching attempt is often unavoidable and is not a foul. If a catching foul occurs and is uncontested, the player fouled gains possession at the point of the infraction. If an uncontested foul occurs in the end zone, the player fouled gains possession at the closest point on the goal line to the infraction. If the marker is stationary, the thrower may not step into them to complete a pass. Strips A defensive player may not knock the disc from the hands of an offensive player. Traveling the offensive player may not drag their pivot foot or run with the disc. A player who is running and catching must try to stop as quickly as possible (3 steps maximum) prior to throwing to a teammate. Donald son, has a focus on outcome studies and basic science with major emphasis on implant retrievals. His ongoing collaboration with Ian Clarke, PhD provides a syner gy between the laboratory and clinical surgical science. To achieve this goal we rely on those individuals who are willing to take on the responsibility, and privilege, to review articles written by their peers. Norman Scott Daniel Allison Jerry Gorski David Mauerhan Raj Sinha Hani Alnakhli Kenneth Greene Michael Mayor Evert Smith Christopher Anderson William Griffn Joseph McCarthy Rami Sorial Asaad Asaad Ronald Hillock Lorcan McGonagle Panayot Tanchev Keith Berend Kirby Hitt Harry McKellop Panayot Tanchev, Jr. Declan Brazil John Ireland Edward McPherson Richard Tarr Warwick Bruce Robert Jamieson Timothy McTighe Jeffery Taylor Hugh Cameron Riyaz Jinnah Jon Minter Robert Thornberry David Campbell Richard Jones Russell Nevins Patrick Treacy Edward Cheal Maurice Jove Steven Nishiyama Allen Turnbull Michael Christie Michael Kaplan Philip Nobel Anthony Unger Ian Clarke Stephen Kayiaros Mary O�Connor Adrian van der Rijt Terry Clyburn John Keggi Julio Palacio Bradley Walter Simon Coffey Kristaps Keggi Christopher Peters William Walter Richard Cook Robert Kennon Derek Pupello Bill Walter Paul Della Torre Louis Keppler Lee Rubin Andrew Wassef Paul DiCesare Stefan Kreuzer Mark Sacaris Richard Welch Thomas Donaldson Lafayette Lage Lewis Samuels Duncan Whitwell Scott Dunitz Jeremy Latham Kent Samuelson Sumesh Zingde C. Your opinion is a critical step to our motivation and overall success, please Editorial Correspondence do not hesitate to communicate with us. Please direct any requests for inclusion, editorial com ments or questions to Timothy McTighe, Dr. The editorial team reserves the right to return manuscripts that have not been submitted in Correspondence accordance with these instructions. Direct any questions regarding the submission process, File Formats or requests for reprints to David Faroo, Director of Com � All articles must be submitted as Word fles (. There is no subscription charge for receipt of this pub � Figures, images, and photographs should be high lication. All illustrations and line art should be at least For information on how to submit articles to the Re 1200 dpi. Articles submitted will need to be divided into separate fles including cover page and manuscript. Submit Articles to the Reconstructive Review � Cover Page includes article title, lists all authors Please visit ReconstructiveReview. All material to be considered for publication should name, their association with the paper, their full post be submitted via this online submission system. Please list all authors in the or Before submitting an article to Reconstructive Review, der that you want them to appear. The manuscript is used in creating the fle for peer review � a double blind process. It is the Correspond Title ing author�s responsibility to ensure that all authors adhere Structured Abstract (Introduction, Materials & to this policy. Methods, Results, Discussion, and Conclusion) There are three statements to choose from on the Dis Introduction closure Statement form, they are: Materials & Methods 1 No benefts or funds were received in direct or indi Results rect support of this article. Once you have prepared your manuscript according Reconstructive Review Production to the information provided above, please go to our web Specifcations site ReconstructiveReview. Once you have registered you will click on the Sub using InDesign running on a Mac. The pub works can be downloaded and shared they cannot be used lisher and editor assume no responsibility for any injury or commercially. The reader is advised to review disclosure stAtement and regard with balance any information published within As part of the online submission process, correspond this publication with regard to any medical claim, surgical ing authors are required to confrm whether they or their technique, product features or indications and contraindi co-authors have any disclosures to declare, and to provide cations. If the Corresponding author is unable to medical physician to review any and all information be confrm this information on behalf of all co-authors, the fore undertaking any change of treatment for their patients. The head office located in Sydney Australia, with offices in Europe and North America.
Buy generic cardarone 200 mg. CARDIOVASCULAR SYSTEM SONG (Circulatory System Song) | Science Music Video.
Despite the fact that Gaines had a low complication rate and good success buy cardarone 200 mg visa cardiovascular disease effects, over two-thirds of the patients had neurapraxic injury to cardarone 200mg discount blood vessels hardening one Vertebrectomy for or both L5 roots and in two this remained permanent cheap 200 mg cardarone amex arteries that supply blood to the brain. This procedure generic 200 mg cardarone coronary heart disease ks4, which a high-grade slip is prone requires a large amount of surgical experience, should only be performed at spe to complications cifically equipped centers. Sacral Dome Osteotomy the main risk of reducing high-grade spondylolisthesis and spondyloptosis is related to the stretching of the L5 nerve roots, which often results in neuropraxia. The sacral dome osteotomy helps to avoid this nerve root injury by shortening of the sacrum. This technique consists of a bilateral osteotomy of the sacral dome, which allows the reduction of the slip without distraction (Fig. This demanding procedure should be carried out Spondylolisthesis Chapter 27 755 a c e Figure 7. Reduction of high-grade spondylolisthesis with sacrum dome osteotomy a the pedicles of L4, L5 and S1 are instrumented with pedicle screws. It is important to note that neu romonitoring is not absolutely reliable, because paresis of the nerve root can occur even hours after the surgery. It is therefore recommended to reduce the slip onlyfarenoughtoallowforagoodsagittalrealignmentandaninterbodybut tressing by a graft or cage (Case Study 2). Complications Typical complications As with all surgical procedures, patients surgically managed for spondylolisthe encountered are neurologic sis must receive the best outcome with low exposure to problems and complica injuries and non-union tions. It is therefore important to appreciate which complications can occur so as to minimize the occurrence and appreciate the psychologic impact these may have on the patient [79]. Depending on the etiology of the condition and the pro cedure performed, complication rates differ significantly. In situ fixation for degenerative low-grade slippage in the adult will have a markedly lower risk of attaining neurologic impairment than complex reconstructive surgery of the adolescent spine in spondyloptosis. As with all neurologic complications, these need to be accurately assessed and diagnostic imaging should occur rap idly. If there is obvious compression of neural structures, be it from hematoma or misplacement of spinal instrumentation, immediate revision surgery should be the consequence. More complex are the cases where there is no radiographic evidence of com pression of neural structures. In cases of only minor deficit, an attentive yet merely observational approach may be warranted. In general for any surgeon, the decision for or against revision surgery is among the most difficult to make. It is therefore prudent to involve a further, less biased surgeon to assess the patient as well as the radiographic parameters and decide for or against revision together. Adjacent segment instability afterinstrumentationmaybeduetoexcessive iatrogenic destabilization of the overlying facet joint and capsule, due to exces sive thinning or complete removal of the overlying lamina or due to degenerative changes to the adjacent motion segment. While the iatrogenic destabilization of a segment certainly will lead to slippage adjacent to a stabilized segment [109], data concerning adjacent segment degeneration are inconsistent. The discussion remains open as to whether these observed degenerative changes reflect the natural history of disc disease or stand in context to the adjacent fusion [66, 83]. As Ogilvie [79] points out, both are probably a factor and therefore as many lumbar levels should be left unfused as are consistent with the goals of surgery. As most slippages are lateral radiographs are the mainstay for the initial as asymptomatic, the true incidence of the condition sessment. Slippage is quan listhesis, rates of around 3%in the general popula tified by either using the method as described by Me tion have been estimated, but depending on the yerding (Grade I�V) or of Taillard (%). Assessment of ethnic group, the incidence may be significantly the sagittal deformity (lumbosacral kyphosis) is cru higher. Treatment decision will stabilizing elements and the disc is confronted with ultimately be based on the age of the patient, excessive shear. The dissociation of the anterior symptoms, etiology as well as the degree of slip and posterior column therefore ultimately results page. General objectives of treatment are to re in slippage, since the disc cannot withstand the lieve pain, reverse neurologic deficit and, in cases of shear forces. Acute pain should be controlled with initial a motion segment, trauma, tumors, and rare syn rest, anti-inflammatory and/or pain-modulating dromes or systemic bone disease. Only those classifications are of true program with paraspinal and abdominal muscle value that are based on anatomy or distinguish be strengthening. If pain does not sufficiently subside, tween developmental and acquired forms of the the use of a brace or orthoses may be beneficial. The two systems which are clinically rele Cast treatment may result in a healing of an acute vant are those of Wiltse/Rothmann and Marchetti/ spondylolysis in selected cases. The Marchetti classification is self-ex planatory and, as it avoids complex terminology, Operative treatment. Back gical techniques is to decompress neural struc and/or leg pain may range from merely harassing to tures, prevent progression and achieve stability severe. Due to technical lolisthesis may develop a sciatic crisis known as the innovations and improvement in implants, there is Phalen-Dixon sign. Tight hamstrings and posture ab an increasing trend to manage spondylolisthesis by normalities accompany the presentation in the ado combined approaches. In the adult patient, mechanical low depend on familiarity with the approach, resources back pain (worse on motion, better on rest) and radi andinfrastructureasw ellasback-upexpertisein culopathy are the prevailing symptoms. Particularly the manage amination may show hyperlordosis of the lumbar ment of high-grade spondylolisthesis is a surgical spine, and in high-grade slippages a step-off be challenge and technically demanding. Patientsshouldbeas with high-grade spondylolisthesis,fusiontoL4is sessed for sensory or motor deficits of nerve roots. Reduction of high-grade spondylo 758 Section Spinal Deformities and Malformations listhesis is still a matter of debate because of the tion, solid fusion and neural decompression are high complication rates associated with these pro more important.