
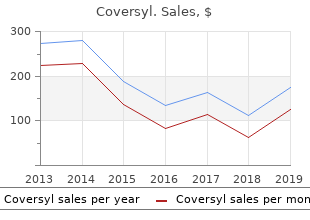
Coversyl
"Discount 4 mg coversyl with amex, medicine 93 3109."
By: Richa Agarwal, MD
- Instructor in the Department of Medicine

https://medicine.duke.edu/faculty/richa-agarwal-md
Removal of electrode(s) may first be attempted by transvenous extraction (code 33244) generic 8 mg coversyl overnight delivery. However buy 4 mg coversyl with visa, if transvenous extraction is unsuccessful best 8 mg coversyl, a thoracotomy may be required to purchase coversyl 4mg visa remove the electrodes (code 33243). Use codes 33212, 33213, 33240 as appropriate in addition to the thoracotomy or endoscopic epicardial lead placement codes to report the insertion of the generator if done by the same physician during the same session. When the "battery" of a pacemaker or pacing cardioverter-defibrillator is changed, it is actually the pulse generator that is changed. Replacement of a pulse generator should be reported with a code for removal of the pulse generator and another code for insertion of a pulse generator. Repositioning of a pacemaker electrode, pacing cardioverter-defibrillator electrode(s), or a left ventricular pacing electrode is reported using 33215 or 33226, as appropriate. Replacement of a pacemaker electrode, pacing cardioverter-defibrillator electrode(s), of a left ventricular pacing electrode is reported using 33206-33208, 33210-33213, or 33224, as appropriate. Tissue ablation, disruption and reconstruction can be accomplished by many methods including surgical incision or through the use of a variety of energy sources (eg, radiofrequency, cryotherapy, microwave, ultrasound, laser). If excision or isolation of the left atrial appendage by any method, including stapling, oversewing, ligation, or plication, is performed in conjunction with any of the atrial Version 2019 Page 103 of 257 Physician Procedure Codes, Section 5 Surgery tissue ablation and reconstruction (maze) procedures (33254-33259, 33265-33266), it is considered part of the procedure. Codes 33254-33256 are only to be reported when there is no concurrently performed procedure that requires median sternotomy or cardiopulmonary bypass. Additional ablation of atrial tissue to eliminate sustained supraventricular dysrhythmias. This must include operative ablation that involves either the right atrium, the atrial septum, or left atrium in continuity with the atrioventricular annulus. A subcutaneous cardiac rhythm monitor is placed using a small parasternal incision followed by insertion of the monitor into a small subcutaneous prepectoral pocket, followed by closure of the incision. Version 2019 Page 107 of 257 Physician Procedure Codes, Section 5 Surgery Procurement of the saphenous vein graft is included in the description of the work for 33510-33516 and should not be reported as a separate service or co-surgery. To report harvesting of a femoropopliteal vein segment, report 35572 in addition to the bypass procedure. When surgical assistant performs graft procurement, add modifier 80 to 33510-33516. To report combined arterial-venous grafts it is necessary to report two codes: 1) the appropriate combined arterial-venous graft code (33517-33523); and 2) the appropriate arterial graft code (33533 33536). Procurement of the saphenous vein graft is included in the description of the work for 33517-33523 and should not be reported as a separate service or co-surgery. To report harvesting of an upper extremity artery, use 35600 in addition to the bypass procedure. When surgical assistant performs arterial and/or venous graft procurement, add modifier -80 to 33517-33523, 33533-33536, as appropriate. The codes include the use of the internal mammary artery, gastroepiploic artery, epigastric artery, radial artery, and arterial conduits procured from other sites. To report combined arterial-venous grafts it is necessary to report two codes: 1) the appropriate arterial graft code (33533-33536); and 2) the appropriate combined arterial-venous graft code (33517 33523). Procurement of the artery for grafting is included in the description of the work for 33533-33536 and should not be reported as a separate service or co-surgery, except when an upper extremity artery (eg, radial artery) is procured. To report harvesting of an upper extremity vein, use 33500 in addition to the bypass procedure. To report harvesting of a femoropopliteal vein segment, report 33572 in addition to the bypass procedure. When surgical assistant performs arterial and/or venous graft procurement, add modifier -80 to 33517-33523, 33533-33536 as appropriate. These codes include all device introduction, manipulation, positioning, and deployment. All balloon angioplasty and/or stent deployment within the target treatment zone for the endoprosthesis, either before or after endograft deployment, are not separately reportable. For fluoroscopic guidance in conjunction with endovascular repair of the thoracic aorta, see codes 75956-75959 as appropriate. Codes 75956 and 75957 include all angiography of the thoracic aorta and its branches for diagnostic imaging prior to deployment of the primary endovascular devices (including all routine components of modular devices), fluoroscopic guidance in the delivery of the endovascular components, and intraprocedural arterial angiography (eg, confirm position, detect endoleak, evaluate runoff). Code 75958 includes the analogous services for placement of each proximal thoracic endovascular extension. Code 75959 includes the analogous services for placement of a distal thoracic endovascular extension(s) placed during a procedure after the primary repair. Other interventional procedures performed at the time of endovascular repair of the descending thoracic aorta should be additionally reported (eg, innominate, carotid, subclavian, visceral, or iliac artery transluminal angioplasty or stenting, arterial embolization, intravascular ultrasound) when performed before or after deployment of the aortic prostheses. Also included is that portion of the operative arteriogram performed by the surgeon, as indicated. To report harvesting of an upper extremity vein, use 35500 in addition to the bypass procedure. To report harvesting of a femoropopliteal vein segment, use 35572 in addition to the bypass procedure. To report harvesting and construction of an autogenous composite graft of two segments from two distant locations, report 35682 in addition to the bypass procedure, for autogenous composite of three or more segments from distant sites, report 35683. These codes are intended for use when the two or more vein segments are harvested from a limb other than that undergoing bypass. Add-on codes 35682 and 35683 are reported in addition to bypass graft codes 35556, 35566, 35571, 35583-35587, as appropriate. Code 35685 should be reported in addition to the primary synthetic bypass graft procedure, when an interposition of venous tissue (vein patch or cuff) is placed at the anastomosis between the synthetic bypass conduit and the involved artery (includes harvest). Code 35686 should be reported in addition to the primary bypass graft procedure, when autogenous vein is used to create a fistula between the tibial or peroneal artery and vein at or beyond the distal bypass anastomosis site of the involved artery.
As was true for Diagnostic nerve biopsies to coversyl 8mg low cost determine the muscle biopsies purchase coversyl 8mg mastercard, the sections submitted for histol cause of a neuropathy are usually obtained as 3 ogy should include both longitudinal and cross to cheap 4 mg coversyl 5-cm-long strips of the sural nerve coversyl 4mg low cost. You should handle these biopsies only should be entirely submitted in formalin for rou when they cannot be handled by a specialized tine paraf? In this manner, margins may be reported as free Skin biopsies comprise a large component of or involved in the planes of section. These biopsies come in many shapes and at least trisect any shave biopsy specimen and sizes, both because of the ease with which 1. Tissue bags or similar aids can the cutaneous surface can be sampled and also help con? Specimens are generally ob tained to diagnose tumors, to ensure complete excision of tumors, and to identify or con? Understanding the suspected diagnosis and pur Many excisional specimens are submitted as el pose of the procedure will help expedite the pro liptical pieces of tissue because this shape leaves cessing of the tissue and ensure an accurate wounds that lie parallel to skin tension lines, diagnosis. That said, excisional specimens can arrive in a variety of other shapes, especially from the face, based on Small Biopsies the anticipated closure. Usu Specimens obtained to establish the diagnosis of ally, there is some indication of how the specimen a cutaneous tumor are usually performed by was oriented. For example, there can be a suture the shave biopsy technique, punch biopsy tech in one tip indicating the superior margin or ink nique, or curettage. Determining the adequacy of placed on one or several surfaces of the tissue resection in fragmented curettage specimens is with an accompanying designation as to orienta not possible. Nonetheless, some same ones used by the surgeon) to allow for accu physicians may request an estimate of tumor ex rate determination of precisely which margins tension to the resection margins, and in fact the are involved or free once the tissue is sectioned. Look for sutures or other markers that the surgeon may have used to help orient the specimen. Submit the centrally located lesion and/or biopsy cavity entirely for histologic evaluation. Multiple tissue sections may be placed in sin On the other hand, perpendicular sections may gle cassettes, but when necessary single slices can miss a positive margin in the remaining tissue be placed in cassettes to allow for more accurate sections. The most reliable approach is to pay determination of the location of resection margins scrupulous attention to the gross appearance of involved with tumor. Most specimens may be the tumor and its relationship to the margins submitted entirely in this fashion. Larger resec when dissecting round and triangular excisional tions for melanoma require sampling of the mar specimens from the skin. In this instance, multi ple samples taken perpendicular to the margin Punch Biopsy of resection and including the tumor (or biopsy wound) are recommended. The deep subcutane the most popular method of skin sampling in ous margin may have to be sampled separately. A core of tissue circumference of especially large elliptical speci is obtained in this manner. Epidermis, dermis, mens may be undertaken as shown in the illustra and subcutis are usually easy to identify, and tion. The biopsy wound, scar, or residual tumor the specimen should be embedded such that is generally centrally located and should be sub tissue sections are obtained perpendicular to the mitted in its entirety. Punch biopsy specimens areas of the specimen are examined, although greater than 0. If the clinician suspects an infectious agent, requesting Round Specimens appropriate special stains at the time tissue is submitted for histology will greatly shorten the Small, round excisional specimens, generally time it takes to diagnose a case. Certain skin conditions display proach to these specimens is to tangentially only subtle or focal histologic? Examples include folliculitis, der specimens are generally separated from the tumor matitis herpetiformis, and transient acantholy by a reliable amount of uninvolved skin. An alternative ap proach is, therefore, to obtain numerous sections Punch Biopsies of the Scalp in radial con? Increasingly, dermatopathologists prefer to inter pret punch biopsy specimens from the scalp, Irregularly Shaped Specimens taken to diagnose in? A similar problem arises in determining ade Perpendicular sectioning results in the identi? The tissue is divided zontal to the epidermis at a level approximately and mounted for frozen sections. Ink and embed mains in the operating suite and the wound is the cut surfaces such that the inked surfaces still anesthetized. The tissue is serially resection margin prompts removal of another sectioned with all tissue placed on slides. We stain plane of tissue only in the involved area(s) and every other slide to reduce the overall number so on until complete removal of tumor is en of slides examined as well as to provide unstained sured. This technique offers a higher cure rate slides for fungal stains if indicated after an initial than conventional procedures and is tissue spar inspection of the tissue. Determination of interface changes at the geon may seek a second opinion regarding the epidermis. The tissue must be processed in horizontal sections, with an effort made to provide anatomic Other Specimens localization of involved margins based on infor mation provided by the clinician. In the face of positive margins, the clinician will reanesthetize Dermatologic surgeons may submit somewhat the (now granulating) wound base and obtain untraditional specimens. Success in this endeavor consist of a variable volume of fat and sero requires exceptionally good communication be sanguineous? While such specimens may be tween the clinician, pathologist, and laboratory submitted as a gross only,? always examine personnel.
It was proposed that the blast population was a lineage buy generic coversyl 8 mg, headed by blast-committed self-renewing stem cells that could also give rise to proven coversyl 4 mg nonproliferative blasts generic coversyl 8mg free shipping. Furthermore order coversyl 8 mg with visa, it was proposed that the blast lineage was derived from leukemic pluripotent stem cells, independently of the committed stem cells that differentiated into normal-appearing myelopoietic lineages. In the model, the pre dominant blast cell population coexisted with minor, but detect able, cells of the granulocytic, megakaryocytic, and lymphoid lineages. This latter conclusion was strengthened by the demon stration that separation of T-lymphocytes from blast cells was necessary for blast colony formation (Minden et al. Col system, in which blasts were cultured in suspension and clonogenic umns show the values obtained at presentation. For stem cells in suspension were considered as self-renewal and could a description, see the text. The discovery and cloning of factors that are required for treated with cytoreductive chemotherapy. When Lan was work colony formation by normal cells in culture provided another ing, cure was rare; after chemotherapy, leukemic clones recov link between the normal and leukemic. A comparison was made factors, it was soon evident that colony formation by blast stem between the culture results seen before treatment and after recov cells required the same stimulation as normal progenitors. The result was clear: no correlation was seen between the other features of blast population, great heterogeneity was seen. Striking synergism was often seen, espe cially when early-acting and late-acting factors are supplied 11. One, karyotype, stands out in every blood used to start the cultures (Dicke et al. With assays on hand, the properties whereas trisomy 8 and deletions of chromosomes 5 and 7 are of the cell of origin of blasts cells were determined. Three properties seemed to It followed that clonogenic blast cells were stem cells that were be candidates: response to growth factors, capacity for self capable both of self-renewal and, through a process analogous to renewal, and sensitivity to chemotherapeutic agents. Any positive normal differentiation, of giving rise to cells that retained the results had to be compared with the strong association between morphology of blasts but had lost proliferative potential. The response of cancer cells to chemotherapy is not reasonable to look for a way to use them in treatment or relate blast necrosis but apoptosis (Gunji et al. Support was obtained from experi enhanced or reduced by such regulators as growth factors and ments in which blast growth was evaluated by measuring uptake retinoic acid. With this assay, about half of blast cell populations did alterations in regulators of apoptosis such as Bcl-2. By contrast, when colony formation in cell recovery; the effect is seen as a change in drug sensitivity culture was used, very few autonomous populations were seen, (Hu et al. These find and no association emerged between response and survival ings are an example of how measurement of a phenotype may (McCulloch et al. Further, growth butes measured in culture never approached the prognostic power factors might reduce the time in aplasia following drug treatment of abnormal karyotypes. Among these, two are not only important and thus decrease the number of early deaths from infection or for prognosis, but also define specific leukemic diseases and bleeding. The break point on chromosome 22 is limited to a tors is to mobilize stem cells from marrow to peripheral blood, small region, termed thebreak point cluster region, or bcr (Groffen where they may be collected with ease for supportive care or trans et al. This protein is a tyro clinical outcome because it was thought that high self-renewal sine kinase, with enhanced activity. Transfer of the bcr/abl gene would be associated with rapid growth and poor prognosis. Lev either in vivo or in vitro causes abnormal stem cell proliferation els of colony formation by cells harvested from primary blast (Groffen et al. The result is a novel measured readily in culture by determining the decrease in colony fusion protein (de the et al. This early evidence was conferred tions could then be sought between D10 and response to drug. Perhaps an explanation of the weak associations might ogy required developing a drug that bound to an important com be that the culture end points were only readily measured responses ponent of the fusion protein, bcr-abl. A large program was to complex regulatory networks, in which other consequences of undertaken looking for tyrosine kinase inhibitors. This mechanism was con haps modified, and then included in the basic knowledge bank that firmed by 3D structural studies that showed the position of is the resource required for further practical developments. In this early work, many of showed convincingly that understanding the proximate molecular these end-stage patients entered remission, and, in some, the lesion in a disease could be used in successful drug development. In contrast to cytotoxic chemotherapy, very few used only by fully trained medical oncologists. The problem faced by the field is not only scientific; it is combined with other antileukemic drugs such as cytosine arabi also economic. Because most cancers have either unique or multiple drugs have already shown both additive and synergistic effects genetic abnormalities, drug development may yield many com (Druker et al. Nonetheless, the abnormal chromosomal trans will not be economical and there will be little motivation to find locations in both diseases are clonal markers. The challenge, then, is not only to use molecular pathology fore, be present in the stem cells that maintain the abnormal clones. Fortunately, history would support the belief that once a principle is established, research and devel 11. The ethical problem arises from the source of such cells? onstration of the clonal nature of spleen colonies derived from trans human embryos. The separation plasticity of adult stem cells contributes to the debate since it might and enrichment of stem cells homing to marrow and spleen on the be argued that these cells could be used in therapy without conflict basis of rhodamine-123 fluorescence. Scientists understand the need for much from single cells: confirmation of assignments by expression profil better information and the long research process that will be needed ing of receptor transcripts. Blood in culture of proliferative blast progenitor cells in acute myeloblastic 53: 1023?1027.
Some requirements of federal law best 8mg coversyl, such as human subjects protections 8mg coversyl for sale, apply to purchase coversyl 8 mg without a prescription state and privately funded stem cell research cheap 4 mg coversyl with visa. For a complete discussion of the mechanisms for oversight of stem cell research, see the National Academies? report Guidelines for Human Embryonic Stem Cell Research. It is legal to conduct research using blastocysts and to derive new cell lines in most states, with some exceptions. Because stem cell legislation is an area of active debate, please visit the National Conference of State Legislatures at. Division on Earth and Life Studies Subscribe to the Earth and Life Studies Gateway at dels. As stem cells have come to the forefront of medical research, the ethical controversies over embryonic stem cells have become prominent. This booklet is designed to provide basic knowledge to facil itate thinking about and understanding the scientific and ethical issues surrounding stem cells. National Academy of Sciences National Academy of Engineering Institute of Medicine National Research Council. The highly specialized cells that make up these tissues originally came from an initial pool of stem cells formed shortly after fertilization. Throughout our lives, we continue to rely on stem cells to replace injured tissues and cells that are lost every day, such as those in our skin, hair, blood and the lining of our gut. Stem cells have two key properties: 1) the ability to self-renew, dividing in a way that makes copies of themselves, and 2) the ability to differentiate, giving rise to the mature types of cells that make up our organs and tissues. Because of their ability to generate multiple, organ-specifc, cell types, they are described as multipotent. Tissue-specifc stem cells have been found in several organs that need to continuously replenish themselves, such as the blood, skin and gut and have even been found in other, less regenerative, organs such as the brain. These types of stem cells represent a very small population and are often buried deep within a given tissue, making them diffcult to identify, isolate and grow in a laboratory setting. Embryonic stem cells can be obtained from the blastocyst, a very early stage of development that consists of a mostly hollow ball of approximately 150-200 cells and is barely visible to the naked eye. At this stage, there are no organs, not even blood, just an inner cell mass? from which embryonic stem cells can be obtained. None of the currently studied embryonic stem cell lines are alone capable of generating a viable embryo. Unlike tissue-specifc (adult) stem cells, embryonic stem cells have the potential to generate every cell type found in the body. Just as importantly, these cells can, under the right conditions, be grown and expanded indefnitely in this unspecialized or undifferentiated? state. These cells help researchers learn about early human developmental processes that are otherwise inaccessible, study diseases and establish strategies that could ultimately lead to therapies designed to replace or restore damaged tissues. It is not yet completely understood how these three to four reprogramming? genes are able to induce pluripotency; this question is the focus of ongoing research. In addition, recent studies have focused on alternative ways of reprogramming cells using methods that are safer for use in clinical settings. Disease-specifc stem cells are powerful tools for studying the cause of a particular disease and then for testing drugs or discovering other approaches to treat or cure that disease. Researchers take what they have learned about how a tissue usually works and what goes wrong in a particular disease or injury and use this information to develop new ways to diagnose, stop or fx what goes wrong. Before being marketed or adopted as standard of care, most treatments are tested through clinical trials. Sometimes, in attempting new surgical techniques or where the disease or condition is rare and does not have a large enough group of people to form a clinical trial, certain treatments might be tried on one or two people, a form of testing sometimes referred to as innovative medicine. For more than 50 years, doctors have been using bone marrow transplants to transfer blood stem cells to patients, and more advanced techniques for collecting blood stem cells are now being used to treat leukemia, lymphoma and several inherited blood disorders. Umbilical cord blood, like bone marrow, is often collected as a source of blood stem cells and in certain cases is being used as an alternative to bone marrow transplantation. Additionally, some bone, skin and corneal diseases or injuries can be treated by grafting tissues that are derived from or maintained by stem cells. For example, the mesenchymal stem cell, found throughout the body including in the bone marrow, can be directed to become bone, cartilage, fat and possibly even muscle. In certain experimental models, these cells also have some ability to modify immune functions. These abilities have created considerable interest in developing ways of using mesenchymal stem cells to treat a range of musculoskeletal abnormalities, cardiac disease and some immune abnormalities such as graft-versus host disease following bone marrow transplant. Identifying, isolating and growing the right kind of stem cell, particularly in the case of rare adult stem cells, are painstaking and diffcult processes. Pluripotent stem cells, such as embryonic stem cells, can be grown indefnitely in the lab and have the advantage of having the potential to become any cell in the body, but these processes are again very complex and must be tightly controlled. In both cases, considerable work remains to be done to ensure that these cells can be isolated and used safely and routinely. Second, as with organ transplants, it is very important to have a close match between the donor tissue and the recipient; the more closely the tissue matches the recipient, the lower the risk of rejection. Being able to avoid the life-long use of immunosuppressants would also be preferable. Third, a system for delivering the cells to the right part of the body must be developed. It contains marrow, but have since been found throughout the body and the inner cell mass, from which embryonic stem cells can give rise to a large number of connective tissue types such as are derived, and an outer layer of cells called the bone, cartilage and fat. Multipotent stem cells Cell line Stem cells that can give rise to several different types of Cells that can be maintained and grown in a dish specialized cells, but in contrast to a pluripotent stem cell, are outside of the body. For example, blood Clinical translation stem cells are multipotent cells that can produce all the different the process of using scientifc knowledge to design, cell types that make up the blood but not the cells of other develop and apply new ways to diagnose, stop or fx organs such as the liver or brain. Pluripotent stem cells Stem cells that can become all the cell types that are found in an Differentiation implanted embryo, fetus or developed organism.
Buy 4mg coversyl overnight delivery. RBG| Blood And Bone REMIX Song by Anxiety X.