
Ventolin
"Generic 100 mcg ventolin mastercard, asthma 4 month old baby."
By: Bertram G. Katzung MD, PhD
- Professor Emeritus, Department of Cellular & Molecular Pharmacology, University of California, San Francisco

http://cmp.ucsf.edu/faculty/bertram-katzung
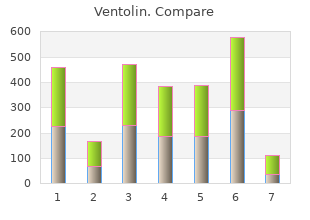
The left hemidiaphragm is usually located one intercostal space lower than the right hemidiaphragm discount ventolin 100 mcg without a prescription asthma in dogs. If one hemidiaphragm is weak buy ventolin 100mcg otc asthmatic bronchitis not getting better, then the normal negative intrathoracic pressure will suck the diaphragm cranially into the thoracic cavity discount 100mcg ventolin overnight delivery asthma 4 year old boy. If the right side is paralyzed generic ventolin 100 mcg otc asthma symptoms 4 dpo, the distance between the right and left diaphragm will be more than two intercostal spaces, and if the left side is paralyzed both hemidiaphragms will appear on the same level (Figure 3). In bilateral weakness, both hemidiaphragms will at a higher level than expected and might be missed on a static chest X-ray. Sometimes a deep costophrenic and craniovertebral angle can be noted due to increased curvature of diaphragm due to its cranial Diseasesdisplacement. Chest X-ray Posterior-Anterior and Lateral view showing right diaphragm located moreChest X-ray Posterior-Anterior and Lateral view showing right diaphragm located more than than 2 intercostal spaces compared to left side. Fluoroscopic test: On tidal breathing in normal individuals, diaphragmatic contraction will lead Fluoroscopic test: On tidal breathing in normal individuals, diaphragmatic contraction will lead to the caudal descent of both hemidiaphragms by at least one intercostal space. On deep breathing or to the caudal descent of both hemidiaphragms by at least one intercostal space. A paralyzed hemidiaphragm will not or snifng, the descent is more pronounced, and is more rapid. A paralyzed hemidiaphragm will show any movements during sniff examination, or can show paradoxical movements in opposite not show any movements during sniff examination, or can show paradoxical movements in opposite directions (video1 supplementary file). Fluoroscopic sniff test requires significant patient effort and directions (video1 supplementary le). Also, due to risks of ionizing radiation on health, this test is being position needed for this procedure. Also, due to risks of ionizing radiation on health, this test is being replaced by an ultrasound examination of the diaphragm. Ultrasound of thorax: the use of ultrasound technology for evaluation of thoracic pathology Ultrasound of thorax: the use of ultrasound technology for evaluation of thoracic pathology has been increasing in the recent time. Ultrasound of diaphragm is noninvasive, simple and can be has been increasing in the recent time. This has replaced the fluoroscopic sniff test as the test of choice especially in young patients be portable. This has replaced the uoroscopic sniff test as the test of choice especially in young due to concerns of cancer due to risk of ionizing radiation by fluoroscopic examination. The patients due to concerns of cancer due to risk of ionizing radiation by uoroscopic examination. The diaphragm appears as a thick echogenic line in M mode ultrasound examination [47]. Diaphragm diaphragm appears as a thick echogenic line in M mode ultrasound examination [47]. Diaphragm thickness varies with inspiratory effort and level of contraction and at total lung capacity it is around thickness varies with inspiratory effort and level of contraction and at total lung capacity it is around 1. During inspiration, inspiration, diaphragmatic muscle contracts and its thickness increase by at least 20% compared to diaphragmatic muscle contracts and its thickness increase by at least 20% compared to its thickness at its thickness at the end of quiet expiration. This dynamic change in its thickness with respiration can the end of quiet expiration. This dynamic change in its thickness with respiration can be measured be measured by using M mode and expressed as percentage change of thickness with deep breathing. Less than Less than 20% increase in diaphragmatic thickness with inspiration suggests diaphragmatic 20% increase in diaphragmatic thickness with inspiration suggests diaphragmatic weakness. As the diaphragm descends to the abdominal cavity with inspiration, reduction in its descent also suggest its weakness (video 2 Supplementary files). In severe weakness, paradoxical movements of the diaphragm can be visualized easily, and can be measured in M mode. In severe weakness, paradoxical movements of the diaphragm can be visualized easily, and can be measured in M mode. For all patients with suspected diaphragmatic palsy, spirometry should be done in both sitting and supine position. In unilateraldiaphragmatic palsy, spirometry should be done in both sitting and supine position. In unilateral hemidiaphragm, forced vital capacity will be reduced by 30% predicted, and in bilateral paralysishemidiaphragm, forced vital capacity will be reduced by 30% predicted, and in bilateral paralysis it it further decreases by 75% predicted. On supine position in normal individuals, the lung functionfurther decreases by 75% predicted. On supine position in normal individuals, the lung function declines by less than 15% due to the restriction of thoracic expansion and external pressure fromdeclines by less than 15% due to the restriction of thoracic expansion and external pressure from abdominal structures. In patients with diaphragmatic palsy, forced vital capacity will further decreaseabdominal structures. In patients with diaphragmatic palsy, forced vital capacity will further by 15% to 20% in unilateral weakness, and 20% to 30% in bilateral weakness (Figuredecrease by 15% to 20% in unilateral weakness, and 20% to 30% in bilateral weakness (Figure 5). This signicant reduction of vital capacity in supine position also correlates with tans-diaphragmaticsignificant reduction of vital capacity in supine position also correlates with tans-diaphragmatic pressure. Residual volume andunilateral weakness and 30% to 50% of that predicted in bilateral weakness. This significant reduction of vital capacity in supine position also correlates with tans-diaphragmatic pressure. Spirometry of patient with bilateral diaphragmatic palsy showing significant drop of lungSpirometry of patient with bilateral diaphragmatic palsy showing signicant drop of lung functions on supine position. Maximum Inspiratory pressure is the pressure recordedMaximum (static) inspiratory pressure. Maximum Inspiratory pressure is the pressure recorded at the mouth during a maximal inspiratory effort against a closed mouthpiece.
For some patients suffering from this condition ventolin 100 mcg without prescription juice asthma treatment, the psychosocial consequences can be many: isolation buy ventolin 100 mcg online asthma symptoms lasting days, 4 buy ventolin 100 mcg low price asthma symptoms hoarseness. As a result of recent scientifc inroads purchase ventolin 100 mcg with amex asthma definition symptoms, new hypotheses have been developed, generating hope that effective treatments will be developed in a not too distant future. This chapter will review current knowledge about the mechanisms identifed to date to explain this syndrome, etiological hypotheses and treatments. Fibromyalgia is a clinical syndrome characterized by diffuse pain, affec resistance. These clinical manifestations are accompanied by a variety of ting the four quadrants of the body (Figure 1), which is experienced symptoms that vary from one patient to another, in terms of quantity, daily, 24 hours a day. Therefore, it is diffcult to categorize people with months in an uninterrupted manner to be recognized as such. It fuctuates in keeping of the opinion that it is more appropriate to speak of a �continuum� in with physiological and emotional stress. It is experienced mainly in the the severity of the clinical manifestations than of specifc sub-groups muscles, joints and skin, but is also often accompanied by visceral pain (Figure 3, page 37). This continuum, moreover, explains why people (for example, intestinal and bladder pain) and occasionally migraines. It does not prevent the individual same pain thresholds, the same constellations of symptoms or the same from moving, walking and occasionally taking part in more intense response to treatments. Fatigue reduces motivation and the ability to initiate a physical the pain affects all four quadrants of the body (upper and lower limbs, activity programme. Inactivity, whether it is associated with a loss of trunk and para-spinal regions). Specifc points (18 tender points) are social function or not, occasionally leads to depressives states. The psychological stresses, this does not mean that the physical symp word �fbromyalgia� is a poorly chosen term. Recent work by Goffaux & done on muscle biopsies have never confrmed a structural anomaly coll. The anomalies identifed in terms phenomena are disturbed in the spines of people with fibromyalgia. All of the studies that have verifed this hypothesis have reached the same conclusions: there Fibromyalgia is not a depression as some clinicians have tried to is no fbromyalgic personality disorder or personality, but simply just lead us to believe. It is true that a signifcant number of people with more common personality traits. The tendency to experience anxiety or fbromyalgia (approximately 40%) develop a depression sooner or later to catastrophize is included among the most frequently identifed traits. In fact, catastrophization encourages hyper-vigilance and leads patients Fibromyalgia must not be confused with other psychiatric into a spiral that merely amplifes the symptoms. Those of three other patients (1, 2 and 3) highlight the importance of the physiological and psychological components of pain. The respective positions of these patients are not necessarily fxed in time, but bilateral shifts are possible. With catastrophization, a fear of movement, a state of hyper-vigilance and a need for fight develops. On the other hand (on the right side), adequate management of fear and exposure to activities is clearly more realistic and part of the road to recovery. Fear of movement/(re)injury in chronic low back pain and its relation to behavioral performance. Patients with fbromyalgia often report an amplifcation of their sensory perceptions (touch, odour, hearing, taste, smell). It is not uncommon to hear someone with fbromyalgia state that they feel more pain throughout their body when inhaling the odour of a cleaning product or the cashiers perfume in a store. A small tap of encouragement on a shoulder and a frm handshake in greeting are often major sources of pain for people with fbromyalgia to the great surprise of the person initiating such a gesture. The hyperexcitability of the skin, muscles and other structures, as peripheral as it may seem, results from physiological and biochemical modifcations in the central nervous system. It is, in particular, the spine and the brain that coordinate and regulate the information contained in pain. Researchers interested in studying these centres have recently identifed anomalies for each of these centres that provide a somewhat better understanding of the phenomena of the perceptual amplifcation of pain. Anomalies in superior centre activity set of sensory and motor functions while working closely with other One the most recently identifed anomalies is that of atrophy of the cerebral nerve structures such as the hypothalamus and the pituitary gray matter in the brain. A team of researchers at McGill University gland, which are involved with the two principal systems that control demonstrated that the loss of gray matter is accelerated in patients with the internal balance of the body: the automatic nervous system (which fbromyalgia as compared to healthy subjects (Kuchinad A & coll 2007). It is, In the case of animal models of diffuse pain, it has been demonstrated moreover, comforting to know that when the pain (or the depression) on numerous occasions that the spinal cord undergoes structural and is controlled in these groups of patients, the gray matter recovers its chemical changes. Certain nerve cells atrophy whereas others multiply initial properties (Rodriguez-Raecke R & coll 2009). The activities of certain ticity� in which the brain re-arranges its own structure under certain excitatory substances and their receptors become increasingly signif conditions (Begley S 2008, Doidge N 2007). Neverthe could also affect the cerebral cortex (and the gray matter) and account less, using indirect means, researchers have been able to demonstrate for the phenomenon described in the previous paragraph. Recourse to approaches based palpitations, dizziness when changing position, sleep disorder, excessive on psychophysical principles (temporal summation of pain) has also led sweating, etc. These latter are called �diffuse noxious inhibitory controls� an internal balance. The sympathetic and parasympathetic nervous systems (called and �inhibitor� systems are in constant equilibrium in the healthy the �autonomic nervous system� because they function autonomously person but that the patient with fbromyalgia suffers from a lack of in the body, without requiring conscious effort) act in a synchronous balance with respect to these two mechanisms (Figure 5).
Generic 100mcg ventolin with visa. Dr Goldstein Discusses Replacement for SIgMID.
These studies (which are described below) are confirming earlier reports that depressive signs and symptoms are common in mania and hypomania cheap 100 mcg ventolin otc asthmatic bronchitis airways, that manic features occur in depres sion effective 100mcg ventolin asthma educator certification, and that mixed states should be conceptualized and defined broadly and dimensionally ventolin 100 mcg discount asthma definition rhetoric, as well as categorically buy 100 mcg ventolin asthma definition journal, and not narrowly. The authors found that depressive symptoms were continu ously rather than bimodally distributed and did not support a clear dichoto mous distinction between dysphoric and non-dysphoric hypomania or mania. They concluded that dimensional as well as categorical approaches were needed to distinguish dysphoric from non-dysphoric states. However, when mixed mania was defined more broadly, differences in sex distribution and hospitaliza tion duration were lost. It was concluded that dimensional rather than categorical systems to describe the degree of associated depression might be a more meaningful method of classifying mania. The authors concluded that the presence of two or more depressive symptoms was a clinically meaningful way to define mixed mania. Dysphoric mood, mood lability, anxiety, guilt, suici dality, and irritability were the only symptoms significantly more common in the mixed group, whereas grandiosity, euphoric mood and pressured speech were significantly more common in the manic,group. They identified five independent factors representing psychomotor pressure, psychosis, increased hedonic function, irritable aggression, and dysphoric mood. The dysphoric mood factor included positive ratings of depressed mood, anxiety, guilt, mood lability, and suicide, and a negative rating of euphoric mood. The authors concluded that the bimodal distribution of the dysphoric mood factor was consistent with the possibility that mixed bipolar disorder was a distinct state. The analysis revealed four factors corresponding to manic activation, depressed state, sleep disturbance, and irritability/paranoia. Cluster analysis separated the patients into two groups, which differed only with respect to depressed mood. Further analy sis, however, suggested three groups of manic patients differing regarding the severity of associated depressive symptoms: mania with minimal depressive symptoms, mania with full superimposed major depression, and mania with depressive symptoms intermediate between the other two. In summary, numerous modern phenomenology studies, including factor-analytic studies, have confirmed the occurrence of depressive symp toms in mania, and have provided support for the hypothesis that mixed mania (mania with depressive features) may be distinct from pure or euphoric mania (mania without depressive features). Moreover, these studies suggest that systems used to define mixed states should be broad and dimensional as well as categorical, rather than overly narrow. Akiskal Goodwin and Jamison (1990) wrote, "in general, it is best to consider the depressive spectrum and the manic spectrum as independent and capable of interacting in a variety of combinations and permutations". Patients can have various combinations of various degrees (none, mild, moderate, severe) of manic and depressive symptoms, thereby allowing more accurate diagnosis and, hence, more appropriate treatment. These observations repeatedly suggest that mixed bipolar states can present as full syndromal depression with subsyn dromal mania, and that modern diagnostic systems should be modified to reflect this. As noted, Kraepelin (1921) described the mood of both depressive or anxious mania and excited depression as often having an anxious component. More recently, factor-analytic studies of the signs and symptoms of mania have found that anxiety loads with depressed mood in mania (Cassidy et al. Kraepelin (1921) noted "the frequent contra diction between the content of the delusions and the colouring of mood. A patient told me with laughing that his nerves were dried up and his blood circulated only as far as his neck. Studies are inconsistent, however, as to whether the overall incidence of psychosis differs between mixed and pure manic states. By contrast, other studies have found higher rates of psychosis in mixed than in pure states. Of 39 patients consecutively admitted for the treatment of mania, all 21 mixed patients had psychotic features compared with 13 (72%) of the 18 � non-mixed patients (p =0. Similarly, defining dysphoric mania as the presence of two or more depressive symptoms, Akiskal et al. Indeed, the reported prevalence rates of mixed states in patients with bipolar disor der from modern studies ranges from 5% (Bauer et al. The wide variability in prevalence rates across different studies is probably due in part to the use of different criteria to define mixed states (McElroy et al. For example, in their study testing five definitions of dysphoric mania and hypomania in 37 outpatients, Bauer et al. In short, rates of mixed mania increase as the degree of depression required for its defini tion decreases. Certain patient populations may be at higher risk than others for experi encing mixed states. Many studies suggest mixed mania may occur more commonly in women than in men, especially when defined by higher degrees of associated depression (Akiskal et al. However, no significant differences have been found between men and women with mixed mania in suicidality, outcome, biological abnormalities, and treatment response (Arnold et al. Childhood and adolescent mania may also be characterized by higher rates of depressive features than is adult mania (Geller and Luby 1997, McElroy et al. Patients with mixed mania have been the mixed bipolar disorders 71 reported to have a younger (Nunn 1979, Post et al. Regarding episode duration, mixed manias have also been reported to be shorter than (Calabrese and Delucchi 1990), equal to (Winokur et al. Data regarding whether or not patients with mixed states experience more episodes of illness than patients without mixed states are inconsistent. From a retrospective chart review of 112 bipolar patients, Nunn reported that mixed-state patients did experience more affective episodes. Studies are also inconsistent as to what types of episodes patients with mixed states have had in the past.
Blackburn qualifies as an author for drafting and revising the manu script for content including medical writing for content 100 mcg ventolin visa asthma definition yeah. Spontaneous resolution of limb dystonia ifies as an author for drafting and revising the manuscript for content and improvement of myoclonus occur in 20% and including medical writing for content cheap 100mcg ventolin with amex asthma symptoms stomach ache. A systematic codes the protein epsilon sarcoglycan discount 100mcg ventolin with visa asthma symptoms 24, is located in review on the diagnosis and treatment of primary (idio chromosome region 7q21 order 100mcg ventolin otc asthma breathing machine. Phenotype Treatment of myoclonus dystonia is symptom genotype correlation in Dutch patients with myoclonus dystonia. Responsiveness to levodopa in drugs including levetiracetam, piracetam, valproic epsilon-sarcoglycan deletions. Pallidal and ventral intermediate thalamic nucleus have been thalamic deep brain stimulation in myoclonus-dystonia. No fasciculations or myokymia were to severe pain, which made breathing uncomfortable seen throughout. Jaiser: spontaneously after 4 to 5 days, leaving him with a Gait and cerebellar function were normal. Past attacks had also Questions for consideration: been precipitated by specific forms of repetitive exer cise such as jogging. Can you interpret the sign demonstrated in the ness in the left leg, but denied any muscle twitching, video What is the differential diagnosis for this There was no significant past medical or family presentation Funding information and disclosures deemedrelevant by the authors, ifany, areprovidedat the end of the article. They may sicandextrinsiclesionsofthespinalcordcould also be absent in obesity, after multiple pregnancies, or produce this picture. This radiologic description would be In the present case, the objective neurologic abnor compatible with either idiopathic syringomyelia or malities were limited to reflex asymmetry and further hydromyelia. Hydromyelia is considered to be a congen investigations should be directed at differentiating ital, static persistence or enlargement of the central spi between syringomyelia and hydromyelia. What additional radiologic investigations might cavity enlargement over time) or electrophysiologic help in terms of prognostication In addition to the structural or sensory changes, and these tend to be of limited causes discussed in section 3, syringomyelia may arise localizing value. By contrast, clinical signs are common as a result of trauma (including iatrogenic trauma), if the cavity has a paracentral extension or is located arachnoiditis/meningitis, and inflammatory myelitis. While not clearly opathic syringomyelia with minimal neurologic deficits defined on examination, the sensory symptoms are should be monitored radiologically and electrophysiolog likely to represent involvement of postsynaptic spino ically at intervals of 3�6 months; significant progression thalamic neurons crossing the midline anteriorly to should prompt consideration of surgical exploration. Spasticity a centromedullary syndrome, manifesting as pain may be controlled with baclofen, tizanidine, or diaze (burning, electric-shock like, radicular) and dissoci pam. Syrinxes can be exacerbated by activities involving ated sensory loss with temperature insensitivity. Spas a Valsalva maneuver, and patients should be counseled ticity, autonomic dysfunction (including Horner to avoid heavy lifting, to minimize coughing, and to ensure regular and soft bowel motions through increased fluid intake and use of laxatives if required. Figure 2 Schematic cross-section of the midthoracic spinal cord Our patient was managed conservatively; carbamaz epine proved ineffective and he opted not to try alter native drugs. Serial assessments at 6-month intervals demonstrated no functional or radiographic changes. Several case series report that idiopathic syringomyelia with minimal neurologic symptoms only progresses in a minority of conservatively managed cases. Jaiser: design/conceptualization of the study, analysis/interpretation of neurophysiology data, drafting/revising the manuscript. Baker: design/ conceptualization of the study, analysis/interpretation of neurophysiology data, drafting/revising the manuscript. Whittaker: analysis/interpretation of neurophysiology data, drafting/revising the manuscript. Chinnery: apse in the substantia gelatinosa, and decussate in the ventral white commissure to ascend drafting/revising the manuscript. The sensory symptoms probably represent a lesion of the postsynaptic spinothalamic S. J Pediatr Orthop 1997;17: pathological correlations in syringomyelia using axial mag 105�108. Experimental syringohydromyelia induced retrospective case series, comprehensive review, and update by adhesive arachnoiditis in the rabbit: changes in the on management. Disclosures deemed relevant by the authors, if any, are provided at the end of this article. Postictal state of complex partial treatment for squamous cell cancer of the neck, due or generalized seizures can result in gait unsteadi to concerns for dehydration. Two weeks after ness associated with fatigue and confusion and stopping the medication, his ataxic attacks re gradual improvement. He also developed severe pounding head or sensory symptoms, and last less than 1 hour. What other historical information is critical for While many types have been described, the most diagnosis How is the clinical diagnosis of episodic ataxia started at age 11 without progressive nature.