
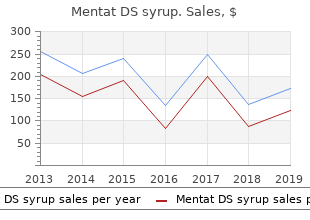
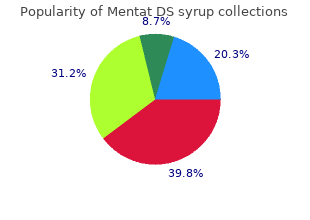
Mentat DS syrup
"Safe mentat ds syrup 100 ml, medications major depression."
By: William A. Weiss, MD, PhD
- Professor, Neurology UCSF Weill Institute for Neurosciences, University of California, San Francisco, San Francisco, CA

https://profiles.ucsf.edu/william.weiss
In addition buy mentat ds syrup 100 ml fast delivery symptoms juvenile diabetes, immune responses need to be quantitatively and qualitatively opti- mal and eventually cease to be operational when the antigen vanishes discount mentat ds syrup 100 ml with amex symptoms 4 dpo. A properly balanced immune response is accomplished by a range of regulatory mechanisms best mentat ds syrup 100 ml treatment wetlands, including a variety of regulatory cells (innate as well as adaptive) (Bach purchase mentat ds syrup 100 ml overnight delivery treatment 6th feb cardiff, 2003; Morelli & Thomson, 2003; von Herrath & Harrison, 2003; Raulet, 2004; Rutella & Lemoli, 2004), the complement system (Carroll, 2004), activation- induced cell death mechanisms (Green et al. Twenty days later, immune alterations are again mostly at control levels, and the effects on the kidney (for instance, proteinuria) are clearly less than on day 10 (Aten et al. Transience of autoimmune effects as well as low- dose protection may both be due to the development of regulatory immune cells. Low-dose pre-exposure to D-penicillamine also induced tolerance in Brown Norway rats (Donker et al. It appeared in this case that low-dose pretreatment prevented all clinical signs of autoimmunity in 60–80% of rats that were sub- sequently treated with a high and usually pathogenic dose of D- penicillamine. Interestingly, low-dose tolerance to D-penicillamine was prevented by poly I:C or lipopolysaccharide treatment (Masson & Uetrecht, 2004). The exact phenotype of the regulatory T cells in the case of low-dose D-penicillamine tolerance is not known, and non-lymphoid cells probably play a role as well. Dose regimen, however, is not the only factor influencing the regulation of autoimmunity. Most drugs are natively not chemically reactive, which means that they cannot form hapten–carrier complexes with proteins or induce release of sequestered or cryptic epitopes (Uetrecht, 1990). They may also be incapable of causing cell damage and inducing subsequent inflammatory signals to stimulate dendritic cells to raise their co-stimulatory molecules or produce stimulatory cytokines. The present thought is that many drugs that cause sensitization undergo bioactivation by metabolizing enzymes (Uetrecht, 1990; Naisbitt et al. This can be accomplished by P450 enzymes, but also by oxidative metabolic routes in phagocytic cells of the immune system, such as polymorphonuclear neutrophils. These cells contain myeloperoxidases that have been shown to be able to convert non-haptenizing chemicals into haptenizing derivatives. However, neutrophils are usually not in close proximity to where sensitization may occur. The list of chemicals dealt with is not comprehensive, nor are the individual examples all exhaus- tively described. The rationale behind selection of the examples is to show the range of agents that are potentially associated with auto- immunity, debates that have been going on for certain agents (e. Although the emphasis is on environmental chemicals, some drugs are exemplified to further address and in fact illustrate the potential autoimmune effects of environmental agents. In less than two years, at least 20 096 people were afflicted by and 356 people died from toxic oil syndrome (Philen et al. Women, especially those less than 40 years of age, were affected more severely than men; 61% of the victims and 66% of the deaths were women (Sanchez-Porro Valades et al. Toxic oil syndrome has strik- ing similarities to autoimmune diseases, particularly scleroderma. In addition, it resembles eosinophilia myalgia syndrome and diffuse fasciitis with eosinophilia. Toxic oil syndrome-associated manifes- tations evolved from initiating vasculitis to eosinophilia in the acute phase and then sicca syndrome, neuropathy, scleroderma, Raynaud phenomenon, and musculoskeletal inflammation in the chronic phase (Kaufman & Krupp, 1995). More than 70% of toxic oil syndrome patients presented with eosinophilia, regardless of age or sex. Chemical analysis of the case-associated oil identified brassicasterol, a marker for rapeseed oil, trace amounts of aniline, oleyl anilide, and other fatty acid anilides and contaminants (Aldridge, 1992; Posada de la Paz et al. The toxin or toxins appear to be stable in oil, since consumption of toxic oil one year after the main epidemic led to development of the disease. Subjective estimates suggest that the degree of illness varied proportionately with the amount and frequency of intake; however, this has not been validated. The initial event is believed to be a form of vasculitis, a non-necrotizing endo- thelial damage in vessels of multiple organs. In the acute phase (0–2 months), patients exhibited endothelial lesions (endovasculitis), eosinophilia, pulmonary infiltrates and oedema, pneumopathy, myal- gias, fever, rash, and high IgE levels (Hard, 2000; Gelpi et al. Aniline was detected in pleural effusion in approximately 50% of the victims (Tabuenca, 1981). Approx- imately 60% of the patients progressed to the intermediate phase (2– 4 months), characterized by myalgias, eosinophilia, cachexia, liver disease, dermal infiltration/oedema, pulmonary hypertension, sicca syndrome, and hypertriglyceridaemia. The primary causes of toxic oil syndrome-related death in this phase were thromboembolism and pulmonary hypertension. Finally, 10–15% of the original toxic oil syndrome cohort have been estimated to progress to the chronic phase (Weatherill et al. In the early stage of the chronic phase (4 months to 2 years), patients developed sicca syndrome, neuropathy, liver disease, scleroderma, and pulmonary hypertension, and then (>2 years) musculoskeletal pain, lung disease, carpal tunnel syndrome, Raynaud phenomenon, and hyperlipidaemia were com- mon. The primary causes of toxic oil syndrome-related death in the 108 Chemical/Physical Agents and Autoimmunity chronic phase were respiratory failure, central nervous system infection, and pulmonary hypertension. While a number of treat- ments were tested, none successfully controlled the disease, although corticosteroids and diphenylhydantoin did ameliorate some of the symptoms (Gomez de la Camara et al. The initial chemical analyses identified oleyl anilide as the primary contaminant and marker for case-associated oils, but the number of anilides and unidentified contaminants suggested that other compounds may also be involved (Posada de la Paz et al. No common refinery products, additives, or contaminants were known to induce symptoms and pathological findings consistent with toxic oil syndrome (Hard, 2002). The oleyl anilide and propanediols were formed by the reaction of aniline with the oleyl side-chain of fatty acids that are abundant in rapeseed oil. Inconsistencies may reflect differences in the stage of the disease at the time of testing. Poly- morphism of this enzyme determines whether acetylation proceeds at a fast or slow rate. Toxic oil syndrome was suggested to be lethal in the acute phase via Th1 mechanisms involving slow acetylation; in the chronic phase, Th2 mechanisms associated with fast acetylation led to autoimmune disease (Cardaba et al.
With blue light the tumour can be seen as pink fluorescence in an area that looked relatively normal with white light generic 100 ml mentat ds syrup visa medicine 2000. This enables the surgeon to see the tumour more clearly during brain surgery and to remove it more accurately discount mentat ds syrup 100 ml with visa medicine video, sparing healthy brain tissue mentat ds syrup 100 ml low cost treatment kitty colds. If the service is for investigative purposes purchase mentat ds syrup 100 ml without prescription medications mothers milk thomas hale, describe the technical specification of the health technology and any reference or “evidentiary” standard that has been established. The viable malignant glioma tumoural tissue is visualised as an intense red fluorescence. This value was defined as the percentage of patients with positive identification of tumoural cells in all biopsies conducted in areas of strong and weak fluorescence. The Gliolan® product information provides details of interactions, use in specific patients, contra-indications, precautions, and adverse events. Indicate whether the service includes a registered trademark with characteristics that distinguish it from any other similar health technology. There are no other products registered for the use in fluorescence guided resection of high grade glioma. Indicate the proposed setting in which the proposed medical service will be delivered and include detail for each of the following as relevant: inpatient private hospital, inpatient public hospital, outpatient clinic, emergency department, consulting rooms, day surgery centre, residential aged care facility, patient’s home, laboratory. Where the proposed medical service will be provided in more than one setting, describe the rationale related to each. This could include details such as frequency of use (per year), duration of use, limitations or restrictions on the medical service or provider, referral arrangements, professional experience required (e. The reconstituted solution is physically-chemically stable for 24 hours at 25ºC, however the product information states that Gliolan® should be used within four hours of reconstitution. Within 24 hours after administration, other potentially hepatotoxic medicinal products should be avoided. Specialised Therapeutics Australia provides neurosurgeons with a distance learning based training program. In addition to these benefits, it is widely accepted that there is a relation between the extent of resection, and survival, in order to provide the best starting platform for adjuvant therapy (Australian Cancer Network 2009). The retrospective study of Lacroix and colleagues (2001), which involved 416 patients with glioblastoma multiforme, identified age, Karnofsky functional status, the degree of necrosis in pre-surgery magnetic resonance imaging, and extent of resection as predictive factors of survival. The prospective study from Albert and colleagues (1994), which included 60 patients with high grade glioma, concluded that patients with a residual tumour had a death risk factor that was six times higher in comparison to patients without residual tumour after surgery. Patients with a complete resection were compared with patients with an incomplete resection, whilst controlling for factors such as age, tumour location and Karnofsky functional status. This re-analysis confirmed the association between the resection degree and survival (Stummer 2008). The treatment of relapses depends on the extension of disease and the patient’s clinical condition. In case of a local relapse, a new surgery is recommended, if possible, either with or without placement of chemotherapy implants. After surgery, patients with a poor functional status only receive supportive treatment, whilst patients with a better clinical condition undergo chemotherapy and/or re-radiation. For recurrence of diffuse pattern or multiple lesions, the therapeutic options are supportive treatment in patients with poor functional status, and systemic chemotherapy and/or surgery for symptomatic relief. These protocols are consistent with the earlier Australian guidleines which recommend concurrent radiotherapy and chemotherapy followed by adjuvant chemotherapy, finding that it provides a significant improvement in median and two-year survival in patients with (Australian Cancer Network 2009). Patients with high grade malignant glioma show symptoms that require appropriate management, namely peritumoural brain oedema, venous thromboembolism and convulsions. The brain oedema causes neurological symptoms that significantly contribute to morbidity associated with the tumour and it is usually treated with corticosteroids (Pace 2010, Stupp et al. Some patients with high grade malignant glioma present a higher risk of venous thromboembolism, and it is estimated that in the first year after diagnosis, 16% to 28% of patients are affected. Treatment with low molecular weight heparin is recommended for 12 patients with symptomatic thromboembolism. Despite the aggressiveness of treatment administered to patients with high grade malignant glioma, the disease remains incurable and patients end up going through a terminal phase with accentuated decline in their clinical condition. The most frequent problems in terminal patients are changes in the state of consciousness, drowsiness, dysphagia, progressive neurological deficits, convulsions, headaches, nausea and vomiting (Oberndorfer 2008, Sizoo 2010, Pace 2009, Pace 2010). It will not affect patients’ eligibility for surgery which is dependent on the lesion not being deeply situated, or diffuse and non-focal, and on the patient’s clinical condition. The expected outcomes for the assessment are: complete resection rate; surgical morbidity; progression-free survival; overall survival; quality of life; reduction in symptoms from mass effect in the brain (headache, neurological deficit); reduced need for corticosteroid, reduction in side effects (used for treatment of brain oedema); and photosensitivity. All magnetic resonances conducted in relation to this study were subjected to revision and centralised evaluation. The evaluation of quality of life in patients with high grade glioma is particularly important due to the impact of the tumour and its treatment on a physical, cognitive and emotional level, and also due to the low life expectancy of these patients. The prospective study by Brown and colleagues (2005) evaluated quality of life in adult patients with recently diagnosed high grade glioma, with the use of questionnaires directed toward general evaluation of quality of life, depression, fatigue and daytime drowsiness. One of the interesting aspects revealed by this study was the existence of statistically significant association between complete resection and improvement in quality of life (p = 0. Within 24 hours after administration, other potentially hepatotoxic medicinal products should be avoided. The proposed economic evaluation is a cost-effectiveness assessment, using a Markov model adapted from that described by Rogers and colleagues (2008) and Garside and colleagues (2007). This model allows calculation of the cost per life year gained, cost per life year gained and adjusted according to quality of life and cost per year gained free of progression.
Discount 100 ml mentat ds syrup with amex. Your Twin Flame Is Thinking About You.
The flap shape has conjunctival flap find that a 6-0 silk suture placed in the no apparent effect on ultimate pressure control discount mentat ds syrup 100 ml on-line symptoms shingles. The anterior margin and sides of a block of limbal sclera are first outlined with a 15-degree blade mentat ds syrup 100 ml sale medications zyprexa. The final step uses Vannas scissors to cut the block free at the scleral spur buy 100 ml mentat ds syrup with amex medicine 665, indicated by E dashed line buy mentat ds syrup 100 ml on line symptoms joint pain fatigue. To reduce the ness and then elevated into clear cornea with a spatula risk of iris prolapse, vertical cuts at the lateral edges are knife, so that iris is visible through the peripheral cornea made first, followed by an incision through the anterior, (Fig. Keeping the tip just phacoemulsification may prefer to make a 4 mm groove inside the anterior chamber, with the sharp edge pointing 3 mm posterior to the limbus and undermine toward the up, and cutting in an upward, horizontal direction allows cornea with an angled spatulated knife, cutting the sides the surgeon to make an accurate cut. This may be neces- of the flap anteriorly up to the limbus at either margin of sary in either direction to ensure that Descemet’s is com- the scleral tunnel (Chapter 44, Fig. With the assistant elevating the scleral flap with a cornea using a 15-degree sharp blade oriented parallel to Colibri-type forceps, the surgeon then cuts the block the iris. This allows subsequent reformation of the ante- completely free at the scleral spur. This is most easily per- rior chamber, either during the procedure or postopera- formed with Vannas scissors, using a vertical cut to avoid tively with balanced salt solution or viscoelastics. Most leaving a shelf of Descemet’s membrane, which could surgeons will apply antimetabolites, discussed in the fol- occlude the sclerectomy. The Kelly Descemet’s punch allows the surgeon the anterior chamber should remain formed, with only a to create the sclerostomy without relying on an slow leak at the flap margins that increases easily with light assistant to hold the scleral flap. If the anterior chamber shallows spontaneously, additional flap sutures are necessary. The sur- geon should never leave the operating room if the anterior With either technique, injecting a viscoelastic into the chamber cannot be easily deepened or does not retain fluid. Unwanted iris prolapse into the sclerectomy can be managed by making a small radial cut with Vannas scis- Surgeons have described several types of releasable sors in the bulging iris, which allows the iris to retract into 16,17,17a 17 sutures. Bleeding from the cut edge of the through the sclera and up through the posterior edge of the sclerectomy, which is common with excessive use of the scleral flap. The needle is then passed back into the scleral Kelly punch posterior to the scleral spur, can be controlled flap more anteriorly, beneath the conjunctival insertion, to with light wet-field cautery. This leaves a loop on top of the scleral also produce a cyclodialysis leading to prolonged hypotomy. A single tie, using four throws of the proximal A peripheral iridectomy prevents iris incarceration in the end of the suture, is then made around the loop on top of fistula. If the pupil is dilated, intracameral injection of the scleral flap and pulled tight. Postoperative removal of acetylcholine (Miochol) will constrict the pupil and facili- this suture involves freeing its corneal end at the slit-lamp tate a basal iridectomy without causing conjuctival hyper- and then pulling downward. With the assistant retracting the scleral flap with knot and frees the entire suture. Gently pulling the iris away from the ative antifibrotic agents requires meticulous, watertight scissors for the beginning of the cut and toward the scissors closure of the conjunctival incision. For limbus-based for the completion of the cut produces an iridectomy that is conjunctival flaps, a two-layer closure of Tenon’s and wider than the sclerectomy (Fig. A curved Vannas conjunctiva, using a running 9-0 Vicryl or 10-0 nylon scissors, held with the curve toward the limbus, provides suture with a lock every 3 to 4 bites, is unlikely to leak. Care Some surgeons prefer a running horizontal mattress tech- is necessary to avoid tearing the iris at its insertion or nique, either in a double layer or a single layer closure including ciliary processes in the iridectomy, as both will that incorporates Tenon’s capsule (Fig. After the iri- either by direct inspection or by “painting” the suture line dectomy, the surgeon should inspect the sclerectomy to with a moistened fluorescein strip. Iris bleeding Fornix-based flaps are closed by suturing the edges of will usually stop following gentle irrigation with balanced conjunctiva to the limbus, pulling the anterior margin taut salt solution or, occasionally, injection of viscoelastic. Attaching the edge of the conjunctiva to rupted 10-0 nylon suture at each corner (Fig. This includes light val buttonhole and injury to the lens and corneal wet-field cautery of episcleral vessels along the outline of endothelium if the needle is passed too deeply into the the scleral flap, and point cautery to bleeding from the anterior chamber. Postoperatively, the externalized suture flap margins, avoiding tissue retraction. Bleeding from an presents a potential wick for bacteria to enter the bleb, iris process or torn iris base following the iridectomy may and blebitis, endophthalmitis, and corneal ulceration have also be controlled with point cautery, or, if necessary, 1% all been reported in eyes with exposed releasable sutures. The timing of laser suture lysis and removal of Antibiotics and corticosteroids are usually adminis- releasable sutures is highly individualized. Neither should tered at the conclusion of surgery, either as a subcon- 20 be performed in the first day or two after surgery if the junctival injection or soaked into a collagen shield. Pred- pressure can be reduced with massage and viscoelastic nisolone drops, begun on the first day after surgery, are material remains in the anterior chamber. Following this, used every 2 hours during waking hours for at least 2 lysis or removal can be performed with good effect up to 2 weeks, and then tapered over the next 4 to 8 weeks. Beyond this, releasable sutures day for 2 weeks, or until removal of releasable sutures. However, antimetabolites can ter, cycloplegics improve patient comfort, deepen the 22 greatly extend the time for effective suture release. Because frail, elderly patients can become confused and disori- Intraoperative and postoperative antimetabolites have ented even with this dosage, homatropine may be safer. Complications of laser suture lysis include hypotony, Black race especially if more than one suture is cut, and damage to the Previous failed filtration surgery conjunctival flap.
To integrate this model we use backward Euler scheme with a unique linearization of F per time step generic 100 ml mentat ds syrup fast delivery medicine 5658. All beam elements being serially connected mentat ds syrup 100 ml generic medicine 7253 pill, F is a tridiagonal matrix with a band size of 12 buy 100 ml mentat ds syrup with mastercard 5 medications for hypertension. Modeling contacts with aneurysm walls Simulating coil embolization requires to accurately model contacts that occur between the coil and the aneurysm wall 100 ml mentat ds syrup sale medicine rap song. The contact model must provide the following features: first, account for the stick and slip transitions that take place during the coil deployment, second include a compliant behavior of vessel wall (we choose the one that is close to Boussinesq model [30]) and finally the friction motion of the coil along the aneurysm wall. For modeling contacts with friction, we use two different laws, based on the contact force and on the relative motion between the coil and the aneurysm walls. The contact law is defined along the normal n and the friction law, along the tangential (t, s) space of the contact. The contact model, based on Signorini’s law, indicates that there is complementarity between the gaps δn and the contact forces fn along the normal direction, that is, 0 ≤ δn ⊥ fn ≥ 0. With the Coulomb’s friction law, the contact force lies within a spacial conical region whose height and direction are given by the normal force, giving two complementarity conditions for stick and slip motion: [δt δs]=0 ⇒ [ft fs] < μ fn (stick condition) t s t s n [δt δs] [δ δ ] = 0 ⇒ [f f ]=−μ f [δt δs] (slip condition) Where the vector [δt δs] provides the relative motion in the tangential space and μ represents the friction coefficient. The obtained complementarity relations could create singular events when it changes from one state to another: For instance, when a collision occurs at instant t, the velocity v(t ) of the coil, at that point, changes instantaneously. The acceleration could then be ill-defined and we can observe some quick changes in the dynamics. Each friction contact creates three non-holonomic constraints along the normal and tangential directions. Our approach allows for processing simultaneously multiple friction contacts, including self-contacts on the coil. Simulation steps the processing of one simulation step begins with solving Equation 1 for all forces except contact forces (f = 0). This free motion corresponds essentially to the deformation of the beam elements under gravity and user force input. Examples of our simulation results: (left) real coil embolization; (right) our simulated coil embolization with 3D coils. This is a complex aspect that influences greatly the overall behavior of the coil model. To describe the mechanical behavior during contact, the mechanical coupling between the different contact points is modeled. This information is provided by evaluating the compliance matrix in the contact space, called W, for both the coil and the aneurysm. Let’s consider a contact α on the node i of the coil (with one constraint along the contact normal n and two along the tangential friction directions t, s). The mechanical coupling of this contact with a contact β (with frame Hβ) on node j can be evaluated with the following 3 × 3 matrix: −1 T M dF dF T W(α,β) = Hα 2 + + Hβ = Hα C(i,j)Hβ, h hdv dq (i,j) where C(i,j) is the 3 × 3 sub-matrix of global compliance matrix C (inverse of tangent matrix) at the rows of node i and the columns of node j. For the aneurysm wall, the formulation of the coupling is simpler: g(dij) T W(α,β) = Hα Hβ, e where e is an elasticity parameter that is homogeneous to young modulus and g(dij) is a Gaussian function of the distance, defined on the surface, between contact point i and j. The Gaussian function allows a fall-off of the coupling with increasing distance between the contact points. This model is close to the Boussinesq approximation which provides a distribution of the normal contact stress from the elasticity of the surface, around a point of contact [30]. The result of the contact response involves finding the friction contact forces that respect Signorini and Coulomb laws. Several works ([18] and [8]) present Gauss-Seidel iterative approaches that solve this problem. The solver needs an evaluation of a global compliance matrix W, which is the sum of the compliances of the coil and the aneurysm wall. It also needs the value of the relative displacement of the contacting points during the free motion δfree. When the contact forces are found, during the last step, called contact correction we compute the motion associated to the contact forces. However, even if the results are quite encouraging, as illustrated in Figure 5, the mechanical modeling is not fully complete. A(Near)Real-TimeSimulationMethodofAneurysmCoilEmbolizationA (Near) Real-Time Simulation Method of Aneurysm Coil Embolization13 235 Moreover, we also aim at predicting the influence of the coils on the hemodynamic status near the aneurysm. As a result, it is important to simulate the flow within the aneurysm, and to propose a method for blood-coil coupling. Modeling of blood flow around intracranial aneurysm the blood is modeled as an incompressible Newtonian fluid of constant density, ρ = 1. In this work, we only consider the blood flow near intracranial aneurysms with relatively small Reynolds number ranging from 100 to 1,000 [31], which satisfies the laminar assumption. Thus, it is reasonable to describe the behavior of blood flow using the incompressible Navier-Stokes equations. Additionally, the influence of pulsating vessel on the fluid is ignored; hence vessel walls are assumed to be rigid. First of all, it is based on unstructured tetrahedral mesh, which is more suitable to describe irregular boundary of anatomical geometries than regular grids. From the tetrahedral mesh, referred as primal mesh, the dual mesh is constructed as follows: dual vertices correspond to the circumcenters of primal tetrahedra, dual edges link dual vertices located on neighbor tetrahedra, and dual faces are surfaces of Voronoi cells of primal vertices, which are dual cells as well. More generally, a dual (n − p)-cell is associated to a corresponding p-simplex (p = 0, 1, 2, 3, n = 3) as depicted in Figure 7. Secondly, the orthogonality between primal and circumcentric dual is useful to define the physical variables in fluid 6), such as flux, which is the face integral of velocity orthogonal to the face, and the vorticity (the circulation per unit area at a point), whose direction is orthogonal to the plane of circulation (the line integral of velocity around a closed curve).