
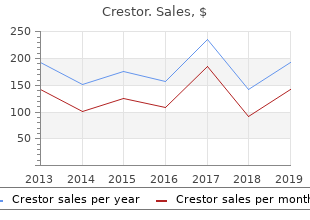
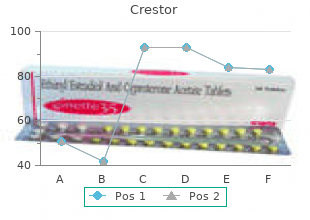
Crestor
"Discount crestor 5mg otc, cholesterol chart diet."
By: William A. Weiss, MD, PhD
- Professor, Neurology UCSF Weill Institute for Neurosciences, University of California, San Francisco, San Francisco, CA

https://profiles.ucsf.edu/william.weiss
Bronchogenic cysts result from abnormal development of the anterior diverticulum of the foregut order 5mg crestor cholesterol raising foods. They com monly are located in the anterior mediastinum or (rarely) in the pulmonary parenchymaandusuallyarenotassociatedwithotherstructuralabnormalities cheap 5mg crestor overnight delivery cholesterol levels hdl ldl. Bronchogenic cysts characteristically present as a single unilocular cyst order crestor 20 mg high cholesterol in eggs myth, with mediastinal shift order crestor 10mg without a prescription cholesterol medication triplex, and evidence of bronchial obstruction. In one case report of antenatal diagnosis, an enlarged, obstructed lung was identied that ultimately led to the discovery of a bronchogenic cyst. Posterior mediastinal neuroenteric cysts occur due to anomalous development of the dorsal foregut and noto chord, probably in the 4th week of gestation. They often are associated with spinal abnormalities and may compress the trachea or communicate with the bowel through a diaphragmatic defect. The most common is posterolateral (Bochdaleck) herniation through the pleuroperitoneal canal or foramen of Bochdaleck. Bochdalek hernias are usually located on the left and comprise up to 92% of diaphragmatic hernia cases. Other potential hernia sites include parasternal (Morgagni) herniation through the costal and sternal originsofthediaphragm;septumtransversumhernias,whichherniatethrough the central tendon; and esophageal hiatal hernias. Diaphragmatic hernias are often fatal (75%), depending on the presence of other associated abnormalities, often as a result of pulmonary hypoplasia or inadequate diaphragmatic musculature for pulmonary function. Infants diagnosed with diaphragmatic hernias should be delivered at a facility that provides intensive care for neonates. Extracorpo real membranous oxygenation is often useful in maintaining the most severely affected of these infants in the peripartum interval. If a feeding vessel from the aorta can be demonstrated, pulmonary sequestration is considered more likely. Two forms of pulmonary sequestra tion have been described: extralobar and intralobar. Extralobar sequestration is more common in prenatal diagnosis than the intralobar variety and is as sociated with increased rates of diaphragmatic hernia, cardiac abnormalities, and gastric duplication. Ninety percent are left sided, located in the poster obasal region in the costophrenic sulcus. Extralobar sequestration results in complete anatomic and physiologic separation or the sequestered structures from other pulmonary structures. The sequestered tissue is surrounded by a separate pleural structure, and drainage occurs via the systemic vasculature, usually the hemiazygous or portal veins. Intralobar sequestration is rare in fetuses but accounts for 75% of sequestrations in children and adults. In in tralobar sequestrations, a portion of the lung is separated from the bronchial tree but it shares a common pleura with the other ipsilateral lung tissue, and venous drainage is usually to pulmonary veins. They haveahighlydisorganizedappearance,oftenwithbothsolidandcysticcompo nents, and are capable of elaborating most body components, including hair, bone, cartilage, muscle, nervous tissue, and other less-differentiated structures. If bone or cartilage are elaborated, they appear highly echogenic when evalu ated with ultrasound. Tracheal or laryngeal atresia in the fetus may result in high degrees of la ryngeal or tracheal obstruction, resulting in trapping of pulmonary secretions within the lungs. The bronchi become distended and lled with trapped secre tions, giving the lungs a hyperechoic appearance bilaterally. Although the femur length is almost always obtained, full measurements of all limbs are rarely performed if there is no concern for underlying skeletal abnormalities or syn dromesaffectinglong-bonedevelopment. Ifabnormallyshapedbonesorshort ened long-bones are observed during the course of a routine sonogram, careful assessment of the long bones is indicated. A rmly established gestational age is essential to properly interpret long-bone measurements. Skeletal Anomalies Evaluationofthefetallimbsanddigitscanyieldimportantinformationrelative to fetal structural abnormalities and the possible presence of syndromic abnor malities or aneuploidy. Chondrodystrophies poten tially detected include the following: Syndrome Rate/livebirths Syndrome Rate/livebirths Achondrogenesis 1/75,000 Hypophosphatasia 1/110,000 (all types) (severe) Camptomelic 1/150,000 Osteogenesis 1/55,000 dysplasia imperfecta Chondrodysplasia 1/85,000 Thanatophoric 1/30,000 punctata dysplasia Whendiminishedfetallong-bonemeasurementsarenoted,itisimportantto distinguish them from symmetric growth retardation. Skeletal dysplasias gen erally are autosomally mediated inherited conditions, while severe symmetric growth retardation also may result from early fetal infections, chromosomal abnormalities, and severe uteroplacental insufciency. Morphologically, most skeletal dysplasias do not affect head circumference, abdominal circumstance, or fetal foot length. Tables that describe average long-bone length for head cir cumference or abdominal circumference or biparietal diameter and gestational age assess symmetry and are useful. They assist in determining whether long bones are small relative to other body characteristics � as in skeletal dysplasia, or whether body proportions are generally symmetric, indicating symmetric growth retardation. It discriminates rather well between chondrodystro phy and symmetric growth retardation because foot length generally is not reduced in chondrodystrophy. If gestational age is known with some accuracy, the relative long-bone length canbeevaluated. These are clinically efcacious criteria, because the degree of long-bone shortening usually is profound in the most skeletal dysplasias. Lesser degrees of shortening of the humerus has also been proposed as a means of screening for chromosomal aberrations. Increased rates of relative shortening of the femur are seen in fetuses with triploidy (60%), Turner syndrome (59%), trisomy 18 (25%), and trisomy 13 (9%).
See main entry homozygous newborn buy 10mg crestor with mastercard ideal cholesterol to hdl ratio, 397 classication of types of purchase 10 mg crestor free shipping cholesterol reducing foods, 268 sympathomimetic purchase crestor 20mg free shipping cholesterol test australia, 292 thanatophoric order 5 mg crestor overnight delivery cholesterol jimmy moore, 394 clinical manifestations, 267�268 tetracycline, 291�292 dysmorphology exam, 228 dened, 267 thalidomide, 283�284 dysplasias dermatosparaxis type, 270 toluene. See main entry morphology by gestational age, left ventricular endocardium in, 458 Vitamin A, 286�287 143�148 microscopic section, 458 Warfarin. See main entry non-forming, trisomies involved in, endocarditis, infective, in newborn, embryos 182 603 17-day: ultrasound, 5 stage 10, 6 endoderm,3,6 5-week: brain: ultrasound, 338 stage 10�12, 8 enterocolitis. See main entry bulbous ngertips, in by week (8 to 26 weeks): mean development time periods of, 660 Rubinstein-Taybi syndrome, values, 663 dicephalus dibrachus dipus (2 heads, 2 239 measurement of, 50 arms, 2 legs), 632 camptodactyly, in Seckel syndrome: per developmental age in previable growth of, serial sonographic ultrasound, 247 fetuses, 663 assessments of, 80�81 early, 12 utility of, 50 hydrocephalic, systemic anomalies in, hyperextensibility of, in Ehlers-Danlos monosomy X, typical appearance, 351 syndrome, 267 331 hydropic, with anemia due to middle, hypertrophy of, in plantar furrows and malpositioned parvovirus, 615 neurobromatosis, 255 toes, trisomy 8, 197 karyotype 45,X, 202 overgrowth of, in Proteus syndrome, Proteus syndrome: dorsal surface, 264 monosomy X 264 Proteus syndrome: sole, 264 with cystic hygromas, 331 overlapping (14-week fetus), 194, 195 rocker-bottom, trisomy 18, 194, 195 with multiloculated cystic syndactyly of second and third, 379 trisomy 21, 187 hygromas, 331 transverse reduction defects, 307 see also toes; polydactyly Pentalogy of Cantrell, 301 webbing of, in Ehlers-Danlos foot plate,10 previable syndrome, 267 foramen of Morgagni, 487 crown-rump length per see also polydactyly foramen ovale, 429 developmental age in, 662 5p syndrome. See focal dermal axial image, 119 uterine fusion abnormalities, 535 hypoplasia chromosomal abnormalities and, vagina, atresia of, 535 gonadal ridge, bipotential, 535 511 see also cervix; gonads; ovaries; testes; gonadoblastoma, 555�556 defects in, 120 uterus gonads dened, 119, 299�300, 497 genito-urinary anomalies and renal aneuploidal effects on, 185 evaluation for, 120 dysplasia, 519 dysgenesis of, types of, 538 illustrated, 498 germ layers, 3�6 embryonic development of, 530�531 incidence of, 119, 510 gestational age removal at autopsy, 60 location of, 510 dened, 13 Gorlin syndrome (basal cell carcinoma neonate with, 300 embryonic morphology by, 143�148 syndrome) ultrasound of, 497 estimating, 310 clefting of face and cutis aplasia in, gastrulation, 25, 220�222 estimations of, 139, 316 385 Gaucher disease estimator of, crown-rump length as, clinical manifestations of, 267 dened, 640�641 13, 84, 139 cranium showing calcication of falx histiocytes in bone marrow aspiration, growth retardation and, 311 cerebri: X-ray, 266 643 measurements used for estimating, dened, 266�267 typical cells, 643 310 granuloma genitalia per growth stage, 2 eosinophilic. See head circumference left atrium morphology, 56 without chromosomal abnormalities, differential diagnostics of, 104�113 left coronary artery, anomalous origin 20 dimensions per fetal month, 669 of, 453 growth plate distorted, 21 left ventricle dened, 391 double-faced (diprosopus), 632 hypoplastic, 73 in asphyxiating thoracic dysplasia, early, 12 ultrasound with color Doppler, type I, 406 ethmocephaly, 191 439 short but histologically normal, 397 posterior, 123 morphology of, 59 posterior fossa view of, 110 non-compaction of, 459 hamartomas shape, altered, 85 with endocardial broelastosis, 452 brous, of infancy, 557�559 thoracic/head-circumference ratio, left ventricular outow view, 135, 464 mesenchymal 127 lesions unidentiable prenatally, 429 dened, 567 head circumference multivalvular, trisomy 18, 195 in newborn, gross appearance, 568 abnormalities, 109�110 opening in situ, 57 incidence of, 567 crown-rump length and, 50 perfusion-xation at autopsy, 68 microscopic appearance, 568 head-circumference/abdominal position abnormalities, 453�456 presentation ndings, 567 circumference ratio, 140 right atrium microscopic appearance, 259 head-circumference/femur-length dilated, in 28-week fetus: hand plates,10 ratio, 109�110, 132, 425 ultrasound, 432 Hand-Schuller-Christian disease. See measurement method for, 51 morphology of, 55 Langerhans cell histocytosis heart right ventricle. See kidneys hypotelorism, 191, 344 in newborn, 518 hydropic infants hypotonia in Zellweger syndrome postmature, 32 anemic, 42 infant, 249 Potter facies from renal agenesis, 516 due to erythroblastosis fetalis, 325 hypoxemia, chronic, 312 short-rib polydactyly dysplasia in laboratory studies in, 184�322 hypoxic ischemic encephalopathy newborn, 409 see also fetal hydrops (H. See abortion, spontaneous sympathomimetic drug use neonatal death and, 42 mitochondrial abnormalities, 651�652 embryopathy from, 292 metal metabolism disorders, 652�655 classication of, 651 limb defects from, 293 metatrophic dysplasia, 396, 398 mitral valve tetracycline use, 291�292 methotrexate, 96�97, 290�291 defect forms, 449�450 trimethadione use, 466 micrencephaly, 355 dysplasia, 432 valproic acid, 287 microcephaly monosomy X. Scientific Report of the 2015 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Health and Human Services and the Secretary of Agriculture. Mention of trade names or commercial products in this report is solely for the purpose of providing specific information and does not imply recommendation or endorsement by the U. Persons with disabilities who require alternative means of communication for program information (e. Additionally, program information may be made available in languages other than English. When appointed a year and a half ago, our Committee accepted the charge of examining where sufficient �new scientific evidence is likely to be available that may inform revisions to the current guidance or suggest new guidance. Dietary Guidelines in forming the basis of Federal nutrition policy and programs and in providing a critical framework for local, state, and national health promotion and disease prevention strategies. We also understood the influence of the Guidelines in shaping policies, standards, and initiatives across the public and private sectors, including public health and health care, education, business, and the food industry and retailers. As such, we approached our review with a broad scope to address the many issues that may be relevant as the government creates the 2015 Dietary Guidelinesfor Americans. In brief, we planned to determine the current composition and quality of the American diet and areas of public health concern; trends in the Nations leading diet and lifestyle-related health problems; the established, measurable impact of overall dietary patterns and physical activity on short and long term health outcomes; the most effective methods of improving dietary patterns and physical activity to achieve favorable health outcomes in Americans 2 years and older; and sound strategies to help promote a healthy, safe, affordable, and sustainable food supply. We also were intent on identifying the Nations major diet and lifestyle-related health disparities and levels of food insecurity in underserved populations. Recognizing the dynamic interplay between individuals, their families and communities, and the environment, we laid out an ecological, systems-based conceptual framework to guide our deliberative processes and then evaluated almost 100 primary and many ancillary research questions. We wish to acknowledge these individuals and their invaluable assistance as we developed our Report. We will be forever grateful for their dedication to working with our expert Committee to create the most productive and wonderfully collegial environment for our deliberations. Our Report highlights the major diet-related health problems we face as a Nation and must reverse. About half of all American adults� 117 million individuals�have one or more preventable chronic diseases that relate to poor quality dietary patterns and physical inactivity, including cardiovascular diseases, hypertension, type 2 diabetes, and diet-related cancers. More than two-thirds of adults and nearly one-third of children and youth are overweight or obese. The dietary patterns of the American public are suboptimal and are causally related to poor individual and population health and higher chronic disease rates. Unfortunately, few improvements in consumers food choices have occurred in recent decades. Under-consumption of vitamin D, calcium, potassium, and fiber are of public health concern for the majority of the U. Furthermore, more than 49 million people in the United States, including nearly 9 million children, live in food insecure households. The economic and social costs of preventable chronic diseases, health disparities, and food insecurity are enormous, and the Nations adverse dietary pattern and physical activity trends must be reversed. Dramatic paradigm shifts arc needed to help individuals and families take more active roles in their personal health and to incentivize health care and public health services, programs, and research to focus more on prevention and personal diet and lifestyle management. We hope our Report will also lead to public policies that align the public and private sectors on common ground to work collaboratively to develop and offer healthier food products and choices, expanded nutrition programs and services focused on prevention, and greater opportunities for increased physical activity. We urge the development and implementation of nutrition and related policies, standards, programs, and services that promote population-wide healthy dietary patterns and physical activity. That said, the Committee wishes to emphasize that the current evidence base has never been stronger and provides a sound basis to guide the development of public policies and effective nutrition and physical activity interventions to promote health and prevent disease at individual and population levels. Establishing the policy framework to achieve these aims is of paramount importance. We look forward to the translation of this Report into future recommendations in the 2015 Dietary Guidelines for Americans. The Committee was charged with examining individual, community, and population levels. The the Dietary Guidelines for Americans, 2010 to Executive Summary ends with a brief summary of this determine topics for which new scientific evidence was chapter. These conditions have been intake; eating behaviors; and the composition of highly prevalent for more than two decades. Second, individual nutrition and physical intake component of the ongoing National Health and activity behaviors and other health-related lifestyle Nutrition Examination Survey. Positive changes in individual diet and examined the prevalence and trends of health physical activity behaviors, and in the environmental conditions that may have a nutritional origin, or where contexts and systems that affect them, could the course of disease may be influenced by diet. For adolescent and individual lifestyle behavior change, food and physical premenopausal females, iron also is a shortfall nutrient.
Schizophrenic crestor 10 mg otc cholesterol levels over 600, schizoaffective and affective disor ders in the elderly: a comparison buy 10mg crestor mastercard lower cholesterol foods eat list. Comparison of long-term outcome of schizo phrenic crestor 20mg cheap cholesterol test san jose, affective and schizoaffective disorders generic crestor 5 mg with amex cholesterol levels lab tests. Pradiktoren der Langzeitprognose von affektiven, schizophrenen und schizoaffektiven Psychosen: Ein Vergleich. Frequency and phenomenology of persisting alter ations in affective, schizoaffective and schizophrenic disorders: a comparison. A study of bipolar (manic-depressive) and unipolar recurrent depressive psychoses. Clinical subtypes of bipolar mixed states: validating a broader European definition in 143 cases. The effect of prophylactic lithium treatment on mortality and suicidal behavior: a review for clinicians. A study in manic-depressive psychosis: clinical, social and genetic investigations. Outcome in mania: a 4-year prospective follow-up of 75 patients utilizing survival analysis. Sleep and circadian rhythms in affective patients isolated from external time cues. Duration of illness prior to hospitalization (onset) in the affective disor ders. A prospective follow-up of patients with bipolar and primary unipolar affective disorder. Manic-depres sive (bipolar) disorder: the course in light of a prospective ten-year follow-up of 131 patients. Unfortunately, according to projections from the Global Burden of Disease report (Jenkins 1997), the global burden of bipolar disorder and other major psychiatric disorders (schizophrenia, major depression, alcohol abuse and dependence, and obsessive�compulsive disorder) will increase by 10. A number of factors contribute to the enormous costs of disability from bipolar disorder. First, bipolar disorder is common and, with an average early age of onset, is frequently a lifelong illness (Weissman et al. For example, estimates from the Cross-National Collaborative Group epidemio logical study indicated that the lifetime prevalence of bipolar disorder ranged from 0. The results of this study also replicated previous findings of an early age of onset of the illness. In addition to being common, bipolar disorder is a recurrent illness; 80�90% of patients with an index manic episode will have subsequent affective episodes (Goodwin and Jamison 1990, Winokur et al. Untreated, the natural course of the illness is towards more frequent epi sodes with shorter intervals of mental health (Goodwin and Jamison 1990). Angst (eds), Bipolar Disorders: 100 years after manic-depressive insanity, 437�448. A third factor contributing to high rates of disability is the lag of functional recovery from an affective episode behind symptomatic recovery. Many weeks and months may separate remission of symptoms and recovery of premorbid functional status (Dion et al. In fact, many patients do not reach full functional recovery and recurrent affective episodes may lead to progressive deterioration in func tioning between episodes (Coryell et al. Thus, disability from bipolar disorder is not simply limited to discrete affective episodes. For example, recent studies provided data regarding the impact of bipolar disorder on voca tional functioning (Kessler and Frank 1997) and marital stability (Kessler et al. Clearly, by these estimates, the personal, social and economic costs of bipolar disorder are staggering. However, economic cost estimates at least provide a means of quantifying the impact of this illness and a means of demonstrating the benefits of effective treatment. In general, costs, in cost-of-illness studies, have typically been defined as core costs resulting directly from the illness and other related costs, including non-health costs of the illness (Rice 1994). Within the core and related cost categories there are direct costs (requiring expenditure of payments) and indirect costs (lost resources) (Rice 1994). Examples of direct costs include funds spent for hospital and nursing-home stays, physician and other professional services, medicines and equipment. In the first study to examine the economic cost of bipolar disorder, Greenberg et al. In their analysis, patients with bipolar disorder in treatment were estimated to have lost approximately 152 million cumulative days from work, and untreated patients an additional 137 million days in 1990. Morbidity costs based on diminished productivity from affective symptoms from bipolar disorder or major depression were $6. For patients with bipolar disorder specifically, impairment was highest in individuals aged 18�24 years. Morbidity costs (in 1985 dollars) were estimated at $137 million for people with bipolar disorder, 18�24 years old; $802 million 25�34 years old; $206 million 36�54 years old; and $18 million 55�64 years old. The authors concluded that "substantial potential cost savings to society could be gained by timely and appropriate treatment interventions to patients suffering from affective disorders" (p. Of the $45 billion total, $7 billion was expended on core costs which included the direct costs of inpatient and outpatient care and other related costs (see Table 1). Indirect costs of $38 billion were substantial, the greatest component of which was lost productivity of wage-earners and homemakers, together totalling $20 billion (Table 1). Thus, the overall cost of treatment of bipolar disorder is only a small portion of its total economic cost and is greatly outweighed by the morbidity and mortality costs of the illness itself.
Levels of evidence were respectively low buy 5mg crestor visa does cholesterol medication make you drowsy, limited for a short-term effect 267 and insufficient for Washington States Departement of Labor and Industries buy 5mg crestor with mastercard cholesterol medication brands. However generic crestor 5 mg with mastercard cholesterol/hdl ratio guidelines, major adverse effects have been reported including burning sensations in the legs during several weeks buy 10mg crestor free shipping cholesterol levels lab values, disc prolapse and development of 269 radicular pain, numbness and paresis resolving after several weeks ; and septic discitis 270 61. A radiofrequency cannula is placed under radiographic guidance in the center of the disc that is heated at temperatures up to 80�C. The device is heated up to 40-70�C, ablating the centre part of the disc and creating a channel. After stopping at a pre-determined depth, the probe is withdrawn, coagulating the tissue as it is removed. Such procedures are generally performed after a positive preliminary facet injection test. Evidence about the effectiveness of radiofrequency facet-denervation is conflicting. Evidence 2 Cost B13 evaluated the effectiveness of the procedure on the basis of one Cochrane 274 275 review and one systematic review. Proper selection of patients and optimal techniques are probably determinant factors to obtain better results. Finally, a comparison between two denervations comes to the following conclusion: there is limited evidence that intra articular denervation of the facet joints is more effective than extra-articular denervation (level 279 C, based on one low quality study ). Boswell et al describe adverse effects such as painful dysesthesias, increased pain due to neuritis or neurogenic inflammation, anesthesia dolorosa, cutaneous hyperesthesia and 61 deafferentation pain. No sensory-motor deficits and no infection in a series of 616 lumbar facet joint radiofrequency lesions performed in 92 patients. Radiofrequency lesioning of dorsal root ganglia Radiofrequency lesioning of dorsal root ganglia is an invasive procedure consisting in partial lesioning of one or several dorsal root ganglia. The rationale for this procedure is that partial lesion of the dorsal root ganglion may reduce nociceptive input at the level of the primary sensory neuron without causing any sensory deficit. This procedure may thus be considered as an alternative to surgical rhizotomy for chronic refractory radicular pain. Radiofrequency lesioning of dorsal root ganglia seems not effective: one good-quality study demonstrated that it was not superior to sham procedure. Radiofrequency neurotomy of sacroiliac joints Radiofrequency neurotomy of sacro-iliac joints is a procedure consisting in denervating the sacro-iliac joint through radiofrequency. Such a hypothesis is evoked when pain relief has been obtained through preliminary sacro-iliac diagnostic blocks with anesthetics or corticoids as described above. Effectiveness of radiofrequency neurotomy of sacro-iliac joints has not been established and its safety is unknown. Evidence 61 Only the guideline of the American Society of Interventional Pain Physicians addresses this procedure. The rationale for this procedure is to inhibit neurons assumed to be involved in the persistence of pain, neurogenic inflammation, muscle 282-285 dysfunction and contracture. This therapy is administered without anesthesia and can be performed on an outpatient basis. However, more good-quality studies should be conducted to reproduce the encouraging results obtained by this team. The safety of the procedure seems good as only minor side effects have been reported. However, these results are limited to three trials conducted by a small number of specially trained and experienced clinicians, in a limited geographical location. Unfortunately, the frequency of such complications is unknown as no study has specifically addressed this issue. This procedure is performed percutaneously or using a spinal endoscope (myeloscope). The rationale for epidural adhesiolysis is to eliminate scar formation, which can prevent direct epidural application of drugs to nerves and other tissues. Hence, instillation of anesthetic drugs, corticosteroids or other substances (hyaluronidase ) is often included in the procedure. Epidural adhesiolysis is generally considered as a technique that should be applied to patients with chronic intractable radicular pain such as the so-called � failed back surgery syndromes �. Effectiveness of epidural adhesiolysis is still debated as evidence about this invasive procedure is very low and conflicting. Safety of the procedure remains unknown: important and frequent complications have been mentioned in case reports. The results of such low-quality studies showed that less than half of the patients reported pain relief after such a procedure. It must be noted that in one of the studies 15% of the patients developed pain aggravation after adhesiolysis. Other references rely on reviews of members of the American Society of American 61 Society of Interventional Pain Physicians. In particular, Boswell distinguishes percutaneous lysis of lumbar epidural adhesions (neurolysis) and endoscopic adhesiolysis (combined with target delivery of steroids). The majority of the remaining studies analyzed heterogeneous groups of patients, most of 61 them with epidural fibrosis consecutive to back surgery. This may cause spinal cord compression, excessive intraspinal and intracranial pressures, epidural hematoma, bleeding, infection, increased intraocular pressures with resultant visual deficiencies and even blindness and dural puncture. Unintended subarachnoid or subdural puncture with injection of local anesthetic or hypertonic saline is one of the major complications of the procedure with catheter adhesiolysis.
Discount crestor 20mg visa. Niacin Flushing Pathway [HD].