
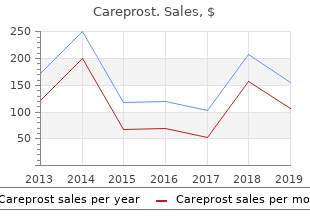
Careprost
"Generic careprost 3 ml free shipping, medicine quinine."
By: William A. Weiss, MD, PhD
- Professor, Neurology UCSF Weill Institute for Neurosciences, University of California, San Francisco, San Francisco, CA

https://profiles.ucsf.edu/william.weiss
Retinal detachment through it separating the sensory retina from the is best examined by indirect ophthalmoscopy pigment epithelium order careprost 3 ml visa symptoms meaning. Cutting of optic nerve Absolute indications Relative indications Separation of conjunctiva and Tenon�s capsule Removal of eyeball purchase careprost 3 ml with amex medicine shoppe. Haemostasis Separation of extraocular muscles Inserting an orbital implant Comprehensive Visual loss buy 3 ml careprost amex symptoms questions. Dark adaptation Visual obscuration in bright light Impairment of colour vision Movement phosphenes and sound induced phosphenes Idiopathic order careprost 3ml on line medicine etodolac. Hereditary optic neuritis Episodic transient obscuration of vision Demyelinating disorders Depth perception, Parainfectious optic neuritis Pain. When the 12 O�clock meridian In pseudostrabismus (apparent squint), the visual of cornea rotates nasally, it is called axes are in fact parallel, but the eyes seem to have a and when it rotates temporally it is called squint: 1. Esophoria is more common in younger age amount of heterophoria is of universal occurrence group as compared to exophoria which is more and is known as. Increased accommo dation is associated with esophoria (as seen in It is a tendency to converge. It may hypermetropes and individuals doing excessive be: near work) and decreased accommodation with i (esophoria greater for exophoria (as seen in simple myopes). Congenital pendular (ocular) nystagmus Acquired ocular nystagmus Tarsal plates and septum orbitale. In general, the serious chemical burns mainly the treatment should be continued for a long comprise alkali and acid burns. If sympathetic ophthalmitis is diagnosed early (during prodromal stage) and immediate Alkali burns are among the most severe chemical treatment with steroids is started, a useful vision may injuries known to the ophthalmologists. However, in advanced cases, prognosis alkalies responsible for burns are: lime, caustic potash is very poor, even after the best treatment. Alkalies dissociate and saponify fatty acids of the cell membrane and, therefore, destroy the structure of cell membrane of the tissues. Being hygroscopic, they extract water from the cells, a factor which contributes to the total uncommon. The above effects result in an increased deep penetration of the alkalies into the tissues. Alkali burns, therefore, spread widely, their action continues for some days and their effects are difficult to circumscribe. In accordence with (Global prospective) are: which many countries have already come up with a Disease prevention and control, �National Blindness Control Programme�. Training of eye health personnel, include: Strengthening of existing eye care infrastructure, 1. Assessment of common blinding disorders at Use of appropriate and affordable technology, local, regional and national levels. Operational research to improve and apply goals of Vision 2020, which are: appropriate technology. Vision 2020 will be implemented through four phases of five year plans, the first one started in 2000 and second in 2005. The is to be placed on achieving: two subsequent phases of implementation will High success rates in terms of restored vision commence from 2010 and 2015, respectively. An information about patient�s the importance of painstaking meticulous history occupation is helpful since ophthalmic manifestations cannot be overemphasized. History of present illness Computer vision syndrome is emerging as a History of past illness significant ocular health problem in computer Family history professionals. Photophthalmitis is known in welders not taking Demographic data should include patient�s name, age, adequate protective measures. In addition, information about the patient�s Name and address are primarily occupation is useful in providing ocular health required for patient�s identification. Recording the religion of the patient may In addition to the utility in patient�s be helpful in ascertaining the diseases which are more identification, knowledge of the age and sex of the common in a particular community. Testing strategies and programes Automated perimeter variables Occlusion of retinal or choroidal vasculature. Loss of vasculature as occurs in patients with choroideremia and myopic degeneration. The electrophysiological tests allow objective evaluation of the retinal functions. It is measured in dark adapted eye with the active electrode (fitted on contact lens) placed on the cornea and the reference electrode attached on the forehead (Fig. Leakage of dye into the neurosensory retina due to a breakdown in inner blood-retinal barrier. The causes are: Blockage of background fluorescence due to abnormal deposits on retina. What inferences are drawn from the movement of the red reflex when concave mirror retinoscope is usedfi While performing retinoscopy, if the shadow appears to swirl around, what does it indicatefi While performing retinoscopy with dilated pupil, one central and another peripheral shadow may be seen. It is the lord of astronomy and the maker of cosmography; it counsels and corrects all the arts of mankind; it leads men to the different parts of the world; it is the prince of mathematics, and the sciences founded on it are absolutely certain. It has measured the distances and sizes of the stars; it has found the elements and their locations; it has given birth to architecture, and to perspective, and to the divine art of painting. The eye is the window of the human body through which it feels its way and enjoys the beauty of the world. Owing to the eye the soul is content to stay in its bodily prison, for without it such bodily prison is torture.
In this case effective careprost 3ml z pak medications, the drug must be l Give 20 mL of 20% magnesium sulfate (4 g) slow intra discontinued until the patellar refex is present generic careprost 3 ml on-line medicine to calm nerves. Otherwise order careprost 3 ml with mastercard symptoms gallstones, venous in 3�5 minutes at a rate not exceeding 1 g/min the plasma level will continue to order 3 ml careprost otc medications safe during breastfeeding increase until a level is Intramuscular loading dose: reached, usually more than 12 mEq/L, where respiratory l 10 mL of 50% magnesium sulfate (5 g) deep intramus depression and respiratory paralysis may ensue. The oxygen saturation usually starts to drop be should immediately follow the intravenous loading dose fore there is evidence of respiratory distress. Patients without convul of respiratory depression induced by hypermagnesemia is sions may receive only the intramuscular loading dose. Ca11 antagonizes the effect of mag nesium by increasing the amount of acetylcholine liberated l Give 5 g magnesium sulfate (10 mL of 50% solution) by the action potentials at the neuromuscular junction. In many cases, decreased oxygen saturation and respira l Urine output should be at least 30 mL/hour or 100 mL in 4 hours tory distress in severe preeclamptic patients receiving mag l Deep tendon reflexes should be present nesium sulfate are not signs of magnesium toxicity, but l Respiration rate should be. In these cases, l Pulse oximetry should be fi 96% the medication of choice is furosemide and the intravenous l Any change in these indices makes it necessary to administration of 20�40 mg of furosemide is usually reevaluate the rate of administration followed by profuse urination and improvement of the Magnesium sulfate is discontinued 24 hours after delivery respiratory distress. The medication may cause maternal death from over dose leading to respiratory failure or pulmonary oedema Chapter | 13 Hypertensive Disorders in Pregnancy 213 and its toxicity is associated with decreased myometrial For the treatment of eclampsia, the loading dosage of activity, slow cervical dilatation, increased blood loss at phenytoin is 10�15 mg/kg. High levels of serum magnesium may depress slowly intravenously, never exceeding a rate of 50 mg/min. Oral administration should dence of myometrial depression has been observed beyond continue for several days during the postpartum period. Magnesium sulfate Antihypertensive Treatment for Acute Management does not affect either the duration of labour or the rate of of Severe Hypertension caesarean delivery. Dangerous hypertension can cause cerebrovascular haemor Maternal administration of magnesium crosses the pla rhage, hypertensive crisis, congestive heart failure, trigger cental barrier and equilibrates in the fetal serum. The objective of antihy respiratory depression and hyporefexia is observed only pertensive treatment in severe preeclampsia is to prevent with severe hypermagnesemia at delivery. Also, there is done during magnesium sulfate administration should be evidence suggesting that antihypertensive treatment may be interpreted cautiously. Chronic hypertension results all, a protective effect of magnesium has been suggested in development of Charcot-Bouchard aneurysms in the deeply against the development of cerebral palsy in very low birth penetrating arteries of the lenticulostriate branch of middle ce infants. These aneurysmal weakening predisposes these Magnesium sulfate acts synergistically with the muscle small arteries to rupture with sudden severe hypertension. Obstetrical anaes Drugs used for rapid lowering of elevated blood pressure thesiologist are aware of this fact and prescribe a smaller in hypertensive crisis are hydralazine, labetalol and nifedipine. Labetalol Labetalol is the medication of choice for treat ment of acute severe hypertension in pregnancy and for Phenytoin Phenytoin has been successfully used for the maintenance treatment of hypertensive disorders during treatment and prophylaxis of eclamptic seizures. The reasons for being the first choice drug are cation is well tolerated and has few side effects. Phenytoin its effectiveness, the low incidence of side effects, and the acts by inhibiting the spread of abnormal activity from the availability of oral and parenteral preparations. The ratio sium sulfate over phenytoin in the prevention of eclamptic of alpha to beta blockade is approximately 1:3 for the oral seizures was demonstrated in a large randomized clinical form and 1:7 for the intravenous form. For intermittent dosing, 20 mg should absorbed after oral administration and reaches peak levels be given intravenous bolus initially over a 2-minute period. The plasma half-life of nifedip Additional doses of 40�80 mg may be given at 20-minute ine is approximately 2 hours. If the blood pressure does not fall into the expected side effect is headaches that may confuse the clinical picture range (diastolic 80�95 mmHg, systolic, 160 mmHg) in in women with preeclampsia. Sudden and severe drops of 20 minutes, the dose in doubled and continued to be dou blood pressure are almost exclusively seen when the capsule bled every 20 minutes until the expected range is obtained is perforated and the medication is applied sublingually. The effective drug is not absorbed through the buccal mucosa but is rapidly dose range is between 50 and 200 mg/hour. The dose varies from patient to patient but usually is the risk of neuromuscular blockade with concomitant between 100�400 mg every 6�12 hours. The blockade may be reversed by the use of 10 mg of intra Hydralazine Hydralazine was commonly used for the venous calcium gluconate. The blood pressure response is almost immedi quently in pregnant women with chronic hypertension and ate. Hydralazine is administered in intravenous boluses, start in gestational hypertension/mild preeclampsia but is not ing at 5 mg and increasing by 5 mg every 20 minutes up to used in severe preeclampsia because of its delayed onset of 20 mg. Reserpine may cause nasal stuffiness in newborns, istration are decreased uteroplacental perfusion and hyperdy which is a rather serious problem because of their obliga namic circulation. Diazoxide plication occurs more often if there is a precipitous drop in the may also cause fetal and maternal hyperglycemia, inhibi diastolic pressure, usually below 80 mmHg. Hyperdynamic circulation after hydralazine administra ally decrease elevated blood pressure. However, cyanide is a tion is a result of its positive inotropic effect and is manifested product of its metabolic degradation and there is a possibility by maternal tachycardia. A meta-analysis of randomized clini of significant fetal toxicity with prolonged administration. Effectiveness of both are simi morbidity and mortality rates as published in fve studies lar. They found serious maternal compli Nifedipine Nifedipine is a calcium channel blocker cations including eclampsia is 16. The accumulated evidence indicates that conservative Nifedipine lowers the blood pressure by inhibiting the intra management for severe preeclampsia developing before cellular influx of calcium into cardiac and vascular smooth 24 weeks is not adequate. Hence in the face of serious Chapter | 13 Hypertensive Disorders in Pregnancy 215 maternal complication approaching almost 50%, it is Expectant Management of Severe Preeclampsia advisable to allow early delivery in these patients with at,34 Weeks Gestation mid-trimester severe preeclampsia to reduce maternal risk Strict patient�s selection criteria and adequate patient and and avoid severe maternal morbidity and prolonged hospi neonatal care facilities are essential to avoid a major disaster talization.
The vestibular system is optimal ly adjusted horizontally and vertically when the head and gaze are directed forward and bent downwards by 30� proven 3ml careprost treatment syphilis. The visual stabilization point then lies about 3 metres in front of a normal adult on level ground discount careprost 3 ml symptoms esophageal cancer. The particular characteristics of the human balance system make it possible to purchase careprost 3 ml without prescription medications related to the lymphatic system com pensate disorders careprost 3ml otc medications similar to gabapentin. In certain kinds of cases, therefore, a repeat examination after one year can be indicated. For employees who suffer from the diseases or functional disorders listed in Section 2. An increased danger of falling at such workplaces is not to be assumed if the em ployees are always secured against falling by technical measures (railings, side pan els, walls, etc. Excerpt Medical, International Congress Series, 1201, Elsevier Publishers, Amsterdam, Lausanne, New York, Oxford, Shannon, Tokyo, 245�260 Claussen C-F, Haralanov S (2002) Cranio-Corpo-Graphy for objective monitoring of alcohol withdrawal syndrome. The prophylaxis aims to prevent adverse effects on health which can be caused by infectious pathogens, or to recognize them at an early stage. This guideline consists of 2 main sections: the first section �Basics� describes the basic examinations and criteria for occupa tional medical assessment and advice on protection from infectious diseases which apply for all activities involving a risk of infection including work in the biotechnol ogy sector. The second section �Specific infections� contains pathogen-specific information and, where relevant, also details of sensitizing or toxic effects. Schedule general medical examination (Basics) special medical examination (Specific infections) medical assessment and advice 394 Guidelines for Occupational Medical Examinations Basics 1 Medical examinations Occupational medical examinations are to be carried out for persons at workplaces involving a risk of infection. Particular at tention is to be paid to disorders of the immune system or to disorders and thera peutic measures which affect the immune system. Follow-up examination � interim anamnesis (including work anamnesis) � medical examination: see initial examination For persons who have been vaccinated against the vaccinable biological agents at the workplace, follow-up examinations are not necessary as long as adequate im munity persists. Final follow-up examination: advice as to conceivable manifestations of disease af ter the end of the incubation period. Histoplasma capsulatum Coxiella burnetii Orthopoxvirus vaccinia Cryptococcus neoformans Orthopoxvirus bovis, O. G 42 2 Occurrence General Adenoviruses are distributed ubiquitously all over the world (man/animals), spo radic, endemic, epidemic; 7 % to 17 % of all intestinal infections, 5 % to 10 % of res piratory infections, epidemic keratoconjunctivitis, locally frequent, outbreaks, mini epidemics, in Germany 138 adenovirus infections (2005), probably a considerable number of unreported cases. Occupational the health service (hospitals, outpatient clinics, ophthalmological practices, commu nal institutions), research establishments, consulting laboratories, social work, metal working industry (�shipyard eye�). Acute respiratory syndrome (serotypes 1�3, 4, 6, 7, 14, 21) Febrile uncharacteristic infections: rhinitis, tonsillitis, laryngitis (serotypes 1�3, 5�7), tracheobronchitis, cervical/preauricular lymphadenopathy; as complications pneu monia (serotypes 1�4, 7), acute otitis media; outbreaks among babies, infants, ado lescents, life-threatening in immunodeficient and immunosuppressed persons. Pharyngoconjunctival fever (serotypes 3, 7, 14) Duration of illness 3�5 days, painful, mostly mild unilateral follicular conjunctivitis (serotypes 3, 4, 7) with cervical lymphadenopathy (swimming pool conjunctivitis), photophobia, lacrimation, inflammation of the plica semilunaris and caruncula lacrimalis, later roundish subepithelial corneal infiltrations; heals mostly without se quelae (often after a period of several months), transiently impaired visus; in severe cases pneumonia (types 1�4, 7); outbreaks among pre-school children, sporadic in adults. Epidemic keratoconjunctivitis (serotypes 8, 19, 37) All age groups, highly contagious nosocomial infections especially in ophthalmolog ical clinics (outpatient and in the wards); favoured by epithelial injury, lacrimal probe, caustic vapours; virus excretion generally in the first two (or three) weeks of illness; mostly unilateral sudden onset, painful follicular conjunctivitis, itching, feeling of a foreign body in the eye, lacrimation, photophobia, inflammation of the plica semilunaris and caruncula lacrimalis, eyelid oedema with ptosis, cervical lymph adenopathy; sometimes after 1 week (20 %�90 % of cases) corneal involvement with whitish subepithelial infiltrations of roundish keratitic foci; symptoms regress after 2�4 weeks, cloudy cornea, mostly heals completely, occasionally impaired visus, haemorrhagic conjunctivitis. Follicular conjunctivitis (serotypes 3, 4, 7) Mild bilateral conjunctivitis (swimming pool conjunctivitis), photophobia, lacrima tion, inflammation of the plica semilunaris and caruncula lacrimalis, later roundish subepithelial corneal infiltrates; accompanied by cervical lymphadenopathy, mostly heals without sequelae (not uncommonly after a period of several months), transient impaired visus; sporadic occurrence or outbreaks (summer). Gastroenteritis (serotypes 31, 40, 41) Second commonest form of viral enteritis in man (after rotavirus enteritis); cardinal symptom diarrhoea (up to 10 days); rarely with raised temperature, vomiting, dehy dration; occasional respiratory symptoms; with mesenteric lymphadenopathy (sero types 1, 2, 5, 6) simulates appendicitis, rare ileac intussusception. G 42 Activities with a risk of infection 403 Acute haemorrhagic cystitis (serotypes 11, 21) Microhaematuria, dysuria, temperature not raised, high blood pressure, normal re nal function, only male babies and infants, self-limiting syndrome. Detection of antigens Immunocytology (swab material) with the direct immunofluorescence test, enzyme im munoassay. Note: under some conditions false positive results for antigen in stool, check positive results perhaps with complement fixation reaction; serotype identifi cation with the neutralization test, haemagglutination inhibition test; Detection of antibodies From week 2 of the illness, confirmation of the diagnosis by taking 2 blood samples 14 days apart: group specific antigens with complement fixation reaction, type specificity with haemagglutination inhibition test, IgM/IgG enzyme immunoassay. After exposure Medicinal therapy: specific therapy not available (antiviral substances are being test ed); otherwise treatment according to symptoms. Occupational Production and use of fungal cultures (moulds) (special laboratories), reference cen tres, consulting laboratories, handling animals, plants or other biological products which are colonized, infected or contaminated; regular contact with infected sam ples or samples suspected of being infected or with contaminated pathogen-contain ing objects or materials, or materials which release fungal elements. Epstein-Barr virus, cytomegaly virus); contact infection via in jured skin or burns, on contact with ornamental and pet birds; endogenous infection (controversial) in persons with persistent immunodeficiency and concomitant patho logical colonization (rare) by allochthonous fungal material; other factors predispos ing to infection: incompetent immune system, diabetes mellitus, long-term wide-spec trum antibiotic therapy, mucoviscidosis, lack of immunity. Other organ involvement After initial colonization of the lungs, haematogenic dissemination or dissemination per continuitatem in predisposed persons: encephalon/meninges: colonization after advanced dissemination or via the nasopharynx, paranasal sinuses, eye sockets, ears; encephalitis (base of brain), meningoencephalitis; paranasal sinuses: maxillary sinusitis; eyes: especially postoperatively in the form of endophthalmitis, choriore tinitis; keratoconjunctivitis (wearers of contact lenses) with involvement of the tear ducts, colonization of the eye socket from the paranasal sinus with destruction of ad jacent bony structures; ears: otomycosis as secondary infection of the external audi tory canal, more frequently with A. After exposure In infected persons, operate on localized processes; for the allergic bronchopulmo nary form glucocorticoids, anti-asthmatics, mucolytics; for the invasive bronchopul monary form and dissemination standard parenteral systemic antimycotic therapy. G 42 Activities with a risk of infection 407 7 Additional notes Any national notification regulations are to be observed. Occupational Research institutes, laboratories (regular work and contact with infected animals/ samples, samples and animals suspected of being infected, other contaminated ob jects or materials containing the infectious agent, given a practicable route of trans mission), veterinary medicine, farming, forestry, hunting, firms and industries pro cessing animal material including transport, work in areas where the disease is endemic. Inhalation anthrax: incubation period up to 5 days (depending on the infection dose), initially symptoms of an acute airway infection; then (within 2�4 days) fulmi nant syndrome: sepsis and/or meningitis, atypical bronchopneumonia with pul monary necrosis; haemorrhagic thoracic lymphadenitis/mediastinitis; shock symp toms; untreated fatal within 3�5 days. Intestinal anthrax: incubation period a few days, raised temperature, dramatic haem orrhagic gastroenteritis with haematemesis, bloody serous diarrhoea, peritonitis (as cites); prognosis unfavourable. Gram stain, direct immunofluorescence test (cap sule) and/or isolation of the pathogen from swab material, sputum, stool, blood. After exposure Isolation of exposed/infected persons generally not necessary; antibiotic therapy in cases of local cutaneous anthrax: ciprofloxacin and penicillin V (7 days); surgical G 42 Activities with a risk of infection 409 procedures contraindicated; in all forms of systemic infections also doxycycline (60 days); when applied in the early phase: fatalities approach 0 % (cutaneous anthrax), 50 % (inhalation anthrax, intestinal anthrax); if the pathogen has been disseminated intentionally. Occupational Facilities for medical examination, treatment and nursing of children and for care of preschool children, care of pregnant women, obstetrics, research institutes, consult ing laboratories. Catarrhal stage Duration 1�2 weeks, prodromal influenza-like symptoms with subfebrile tempera tures. Stadium decrementi Duration 6�10 weeks, gradual decrease in coughing attacks; intercurrent respiratory infections can cause a recurrence of clinical symptoms. Complications Mainly in the first year of life; about 25 % bacterial aspiration pneumonia, respon sible for half of the deaths, secondary infections (H. Borrelia burgdorferi, Borrelia burgdorferi sensu lato 1 Infectious agent Flexible Gram-negative spirochaete, sensitive to environmental factors; complex of human pathogens in Europe includes the species Borrelia (B. Occupational Farming, forestry and timber industry, gardening, kindergartens in the woods, re search institutes, reference centres, regular work in low vegetation and in woods.
Women with syphilis should be queried about illicit substance use cheap 3ml careprost overnight delivery treatment bee sting, espe cially cocaine purchase careprost 3ml overnight delivery treatment zone guiseley. Results of the maternal serologic tests and treatment discount careprost 3 ml on-line medications migraine headaches, if given quality careprost 3ml symptoms 6dp5dt, should be recorded in the neonate�s medical record or be made available to the neonate�s pediatrician. Management decisions are based on the three possible maternal situations: 1) maternal treatment before pregnancy, 2) adequate maternal treatment and response during pregnancy, or 3) inad equate maternal treatment or inadequate maternal response to treatment (or reinfection) during pregnancy. The dosage should be based on chronologic age rather than gestational age and is 50,000 units/kg, intravenously, every 12 hours (for infants 1 week of age or younger) or every 8 hours (for infants older than 1 week). Alternatively, procaine penicillin G, 50,000 units/kg, intramuscularly, can be administered as a single daily dose for 10 days; no treatment failures have occurred with this formulation despite its low cerebrospinal fluid concentrations. For example, a titer of 1:64 is fourfold greater than a titer of 1:16, and a titer of 1:4 is fourfold lower than a titer of 1:16. If a single dose of benzathine penicillin G is used, then the infant must be fully evaluated, full evaluation must be nor mal, and follow-up must be certain. When possible, a full 10-day course of penicillin is preferred, even if ampicillin initially was provided for pos sible sepsis. Use of agents other than penicillin requires close serologic follow-up to assess adequacy of therapy. Infants who have a normal physical examination and a serum quantitative nontreponemal serologic titer either the same as or less than fourfold (eg, 1:4 is fourfold lower than 1:16) the maternal titer are at minimal risk of syphilis if they are born to mothers who completed appropriate penicillin treatment for syphilis during pregnancy and more than 4 weeks before delivery, and if the mother had no evidence of reinfection or relapse. Although a full evaluation may be unnecessary, these infants should be treated with a single intramuscular injection of penicillin G benzathine because fetal treatment failure can occur despite adequate maternal treatment during pregnancy. Some experts, however, would treat with penicillin G benzathine as a single intramuscular injection if follow-up is uncertain. Lyme Disease Lyme disease is caused by a spirochete (Borrelia burgdorferi) transmitted by the bite of a deer tick. A late manifestation of Lyme disease is relapsing arthritis, usually pauciarticular and affecting large joints. The neonate�s health care provider should be informed when maternal disease is suspected. For women who are allergic to penicillin, erythromycin is recommended for 2�3 weeks. If entrance into such areas is necessary, long-sleeved shirts and long pants tucked in at the ankle are helpful. Prophylactic antibiotic therapy for deer tick bites is not rec ommended routinely. Perinatal Infections 433 Parasitic Infections Malaria Although malaria mainly is confined to tropical areas of Africa, Asia, and Latin America, international travel and migration have made malaria a disease to con sider in developed countries. Malaria infection may be more severe in pregnant women and also may increase the risk of adverse outcomes of pregnancy, including spontaneous abortion, stillbirth, preterm birth, and low birth weight. Because of the risk to both the woman and the fetus, and because no chemoprophylactic regimen is completely effective, pregnant women (or women likely to become pregnant) should avoid travel to malaria-endemic areas. Definitive diagnosis (of the mother and the infant) relies on identifica tion of the parasite on stained blood films. Signs of congenital infection at birth may include maculopapular rash, generalized lymphadenopathy, hepatosplenomegaly, chorioretinitis, hydroceph aly, microcephaly, and intracranial calcifications. Because the presence of antibodies before pregnancy indicates immunity, the appropriate time to test for immunity to toxoplasmosis in women at risk is before conception. The diagnosis of maternal infection is based on serologic test results for the detection of Toxoplasma-specific antibodies. In addition, false-positive test results are common with commercially available kits. Food and Drug Administration after serologic confirmation at a reference laboratory; it is recommended for pregnant women at risk unless fetal infec tion is documented. Congenital toxoplasmosis can be diagnosed serologically by the detection of anti�toxoplas ma-specific IgM or immunoglobulin A antibodies soon after birth or by the persistence of anti-toxoplasma IgG beyond 12 months of age. If the diagnosis is suspected (but unconfirmed) at the time of birth, ophthalmologic, auditory, and neurologic examinations should be performed. Acyclovir prophylaxis to pre vent herpes simplex virus recurrence at delivery: a systematic review. Update on immunization and pregnancy: tetanus, diphtheria, and pertussis vaccination. However, when coloni zation with certain organisms occurs, the outcome may be devastating for the neonate, the mother, or both. Many of the nosocomial infections that occur in intensive care units are caused by pathogens acquired from the hospital environ ment (ie, health care-associated infections). Health care-associated infections result in increased morbidity and mortality, prolonged lengths of hospital stay, and increased medical costs. Definition of Health Care-Associated Infection Health care-associated infection is defined as an infection that is acquired in the hospital while receiving treatment for other conditions. The infection-control committee of each hospital should work with perinatal care personnel to ensure that appropriate surveillance of health care-associated infection is being performed. This includes cleaning and decontamination of the environment, using meticulous patient care tech niques, practicing hand hygiene, promoting breastfeeding (unless contraindi cated because of maternal infection; see also �Contraindications to Breastfeeding� in Chapter 8), limiting the number of invasive procedures (eg, central lines), limiting the number of visitors, grouping together (cohorting) infants colonized with the same pathogen, the judicious use of antimicrobial therapy. Labor and Delivery Admission Policy the pediatric health care provider should be notified of all mothers admitted to the antepartum obstetrics unit who are colonized with or are chronic car riers of a potentially infectious organism that may be transmitted vertically to the neonate (eg, human immunodeficiency virus, hepatitis B or hepatitis C virus, herpes simplex virus, influenza, methicillin-resistant staphylococcus, vancomycin-resistant enterococcus) or may be associated with a congenital infection.
Cheap 3 ml careprost fast delivery. Survivor series: She had sore throat symptoms and everyone thought that she was HIV positive.