
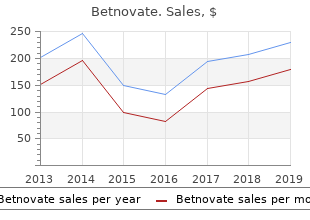
Betnovate
"Order betnovate 20 gm amex, acne 3 step."
By: Richa Agarwal, MD
- Instructor in the Department of Medicine

https://medicine.duke.edu/faculty/richa-agarwal-md
Posteriorly purchase betnovate 20gm acne kit, the back of the bony orbit order betnovate 20gm with visa acne jeans men, which is accounted for by the sphenoid generic betnovate 20gm otc acne prescription medication, can be seen (arrows) buy betnovate 20gm with amex skin care kemayoran. Hence, in practice, the view used for the assess ment of the orbits with a lateral approach represents a slightly oblique view of the fetal head (Figure 3. The lat median aspects of the orbits are clearly visible, which eral walls of the orbits and the midline structures (ethmoid) are allows correct measurement of binocular and interocu clearly displayed. It should be emphasized that the above case, though they are better displayed with a ventral approach mentioned measurement does not represent an integral (see Figure 3. However, orbital view can also be achieved as a perfectly axial plane, it is biometry should be checked whenever there is a sus common practice to obtain it with a minimal rotation picion of orbital malformations such as hypertelorism, of the transducer and that insonates the anterior aspect hypotelorism, or microphthalmia. As has been said, this view should be bulbs, regardless of how normal or abnormal they may sought to assess the intraocular soft tissues, the lenses, appear on this view, should be electively assessed on and the posterior walls of the orbits, represented the ventral approach view (see below). Consequently, this decided to describe the two views separately, in order represents the elective approach for the diagnosis of to underscore the different accuracy with which the lens and ocular abnormalities; in addition, because the soft and hard tissues of the bony orbit and ocular bulb two nasal bones also are visible in cross-section, severe are displayed in each. The alveoli of the upper teeth are positioned sym the oropharynx (arrows) is visualized posteriorly, in the prever metrically in relation to the midline and the maxillary sinuses. Lateral to the tongue, the two mandibular rami are In front of the upper alveolar ridge, the upper lip, displayed seen in cross-section (arrowheads). This plane cuts through the reliable methods to detect also moderate micrognathia hard palate and the upper alveolar ridge, allowing the are the Jaw Index and the Inferior Facial Index. Therefore, in this view, the plane, which consists of an axial view of the fetal neck tongue diameters [6] can be measured in order to arrive at the level of this gland, is relatively difficult to obtain, at a diagnosis of macro or microglossia. Turricephaly, due to early closure of the coronal suture, is typical of Apert syndrome (acrocephalosyndactyly). In the case of a bilateral cleft lip/palate, there is commonly additional tissue on the philtrum, which becomes evident on the midsagittal view Figure 3. Mild macroglossia can be found in trisomy roid (T) appears as a weakly hyperechoic midline round struc 21 (Down syndrome), whereas severe macroglossia is typical of ture surrounding the trachea (reference dot). This view, which is an the thyroid, which surrounds the trachea, is seen in the extremely important one to obtain in order to get center of the neck between the two jugular veins and an overall idea of the anatomic proportions of the carotid arteries, with the cervical vertebra posteriorly fetal face, represents a midsagittal plane, as already (Figure 3. Its importance is due to the fact that in diagnose the rare cases of fetal goiter or neck tumors. In this dimensional ultrasound, allows visualization of the external view, the following structures can be recognized: the frontal ear, which is abnormal or wrinkled in some syndromic condi area, the nasal root, the nose with the nasal bone (arrow), the tions. This lips with the bony palate (bp) in cross-section, and the chin, image was obtained in a 29-week-old fetus. It should be noted that if the view is perfectly on the midline, as in this case, the orbits cannot be seen, this being a symmetric organ. In addition, a wide nasal root, is mainly based on a subjective due to the yet-unossifed metopic suture, the ultrasound beam assessment. The irregularity and the extreme pheno slightly over the lower one; and the chin with the typic variability of the lines that make up the human bony mandible. It is useful to note that, if the scanning face do not lend themselves easily to the creation of view is perfectly on the midline, the insonating beam nomograms expressing the harmony and the correct passes through the still open metopic suture, allowing mathematical or geometric relationships of the vari a nice view of the brain, with the corpus callosum, the ous elements composing the facial profile at least in cavum septi pellucidi, the third ventricle, the quadri the fetus [1]. Consequently, the diagnosis of generic geminal plate, and the cerebellar vermis (Figure 3. The structures, such as the eyes in the case of proptosis, most lateral sagittal plane of the fetal head is that bilateral cleft lip (additional tissue on the philtrum), or passing for the external ear, which can be insonated the tongue (macroglossia). It is difficult to confirm a diagnosis of low-set ears, Lips (oblique) and related malformations. Oblique tan frequently associated with chromosomal abnormali gential views of the lips and palate are of fundamental ties and nonchromosomal syndromes, but it is possi importance for the detection of facial clefts and abnor ble to confidently detect preauricular tags, which are malities of the nostrils associated with the holoprosen also associated with rare syndromic conditions [10]. An oblique However, it should be emphasized that this parasagittal view of the lips allows assessment of the philtrum in the two-dimensional (2D) view has been replaced by the middle of the upper lip, its relationship with the nostrils, 3D surface-rendering image of the fetal face, which is the lower lip, and, inferiorly, the chin (Figure 3. In this cor is parallel but deeper in comparison with the previous onal view, the fetal splanchnocranium is displayed en one (see Figure 3. It allows assessment of the upper face, allowing an overall evaluation of the various ana alveolar ridge and, therefore, detection of defects of the tomic structures (Figure 3. At the same time, this hard palate and their relationships with the nasal cavity allows recognition of abnormally protruding anatomic (Figure 3. The most signifcant malformations detectable on this view are as follows: � Single nostril: Midline defect, associated with the holoprosencephaly sequence � Median cleft: Midline defect, associated with the holoprosencephaly sequence � Unilateral cleft lip/palate: Unilateral defect of the lip, alveolar ridge, and hard palate � Bilateral cleft lip/palate: Bilateral defect of the lip, the alveolar ridge, and hard palate, commonly associ ated with additional tissue on the philtrum Artifacts In such a circumstance, it is necessary to reobtain Orbits. Because the orbits are symmetric organs, the plane, making delicate sweeping and tilting care should be taken to obtain a perfectly axial movements, in order to achieve a correct symmetric view. If this does not happen, a false-positive diag positioning of the transducer to remove the artifact nosis of microphthalmia can be made (Figure 3. A false-positive diagnosis of microph thalmia can be made if the plane for the visualization of the orbits is not perfectly axial. This fgure illustrates the level of the scanning plane and the corresponding two dimensional ultrasound image. If the umbilical cord lies close to the upper lip, move or, better, to switch on color/power Doppler to identify this can sometimes create the false impression of a the umbilical blood fow and remove the artifact. In this case, the lips should be checked again after a few minutes, to allow the frequency) may be used to discriminate between fetus to move. Alternatively, power Doppler (or the cord lying on the lips and a real cleft lip/palate color Doppler with a relatively low pulse repetition (Figure 3.
The concentrations of xanthine and hypoxanthine in cerebrospinal fluid as therapeutic guides in hydrocephalus 20gm betnovate otc acne extraction. Catechol estrogen metabolites and conjugates in different regions of the prostate of Noble rats treated with 4-hydroxyestradiol: Implications for estrogen induced initiation of prostate cancer 20 gm betnovate otc acne xenia gel. Molecular origin of cancer: Catechol estrogen-3 purchase betnovate 20gm without a prescription acne around nose,4-quinones as endogenous tumor initiators generic betnovate 20gm with visa acne and birth control. Neurochemical changes in the rat brain after intraventricular administration of tryptamine-4,5-dione. Vitamin C suppresses oxidative lipid damage in vivo, even in the presence of iron overload. Determination of 15N isotopic enrichment and concentrations of allantoin and uric acid in urine by gas chromatography/mass spectrometry. Evaluation of plasma low molecular weight antioxidant capacity by cyclic voltammetry. Determination of six indolic compounds, including melatonin, in rat pineal using high-performance liquid chromatography with serial fluorometric-electrochemical detection. L-ascorbic acid quenching of singlet delta molecular oxygen in aqueous media: Generalized antioxidant property of vitamin C. Antioxidant activities of some tryptophan metabolites: possible implication for inflammatory diseases. Oxidation of 3-hydroxyanthranilic acid to the phenoxazinone cinnabarinic acid by peroxyl radicals and by compound I of peroxidases and catalases. Inhibition by interferon-gamma of human mononuclear cell-mediated low-density lipoprotein oxidation. Efficacy of dietary d-alpha-tocopherol and dl-tocopheryl acetate for weanling pigs. A modified catalase assay suitable for a plate reader and for the analysis of brain cultures. Scavenging effect of silipide, a new silybin phospholipid complex, on ethanol-derived free radicals. The risk of developing lung cancer associated with antioxidants in the blood: Ascorbic acid, carotenoids, tocopherol, selenium, and total peroxyl radical absorbing capacity. Glutathione and ascorbate during ischemia and post-ischemia reperfusion in rat brain. The relationship of intracellular iron chelation to the inhibition of regeneration of human ribonucleotide reductase. Structure-activity relationship and classification of flavonoids as inhibitors of xanthine oxidase and superoxide scavengers. Protective effects of melatonin in zymosan-activated plasma-induced paw inflammation. N-acetylcysteine: Pharmacological considerations and experimental and clinical applications. The failure of aerosolized superoxide dismutase to modify pulmonary oxygen toxicity. Oxidative stress and abnormal cholesterol metabolism in patients with adult respiratory distress syndrome. Melatonin counteracts lipid peroxidation induced by carbon tetrachloride but does not restore glucose-6-phosphatase activity. Protection of Chinese hamster ovary cells from paraquat mediated cytotoxicity by a low molecular weight mimic of superoxide dismutase. Decreased total antioxidant capacity of normal lipid hydroperoxide concentrations in sera of critically ill patients. Oxidation of melatonin by singlet molecular oxygen produces N1-acetyl-N2-formyl-5-methoxykynurenine. Tissue injury by reactive oxygen species and the protective effects of flavonoids. Analysis of hepatic reduced glutathione, cysteine, and homocysteine by cation-exchange high-performance liquid chromatography with electrochemical detection. Desferrioxamine inhibition of the hydroxyl radical like reactivity of peroxynitrite: Role of the hydroxamic groups. Total homocysteine level in plasma: High performance liquid chromatographic determination with electrochemical detection and glassy carbon electrode. Determination of dehydroascorbic acid using high-performance liquid chromatography with coulometric electrochemical detection. Isocratic reversed-phase liquid chromatography of all-trans-retinoic acid and its major metabolites in new potential supplementary test systems for development toxicology. Will the �good fairies� please prove to us that vitamin E lessens human degenerative disease Bilirubin, formed by activation of heme oxygenase-2, protects neurons against oxidative stress injury. Microdialysis of melatonin in the rat pineal gland: Methodology and pharmacological applications. Parasympathetic inhibition of pineal indole metabolism by prejunctional modulation of noradrenaline release. Exogenous melatonin entrains rhythm and reduces amplitude of endogenous melatonin; An in vivo microdialysis study. Microdialysis reveals dynamics of coupling between noradrenaline release and melatonin secretion in conscious rats. Anethole dithiolethione prevents oxidative damage in glutathione depleted astrocytes. Melatonin in edible plants identified by radioimmunoassay and by high-performance liquid chromatography-mass spectrometry.
Depression of the diaphragm on the side of the pneumothorax (with tension pneumothorax) buy 20 gm betnovate mastercard acne 10 dpo. Displacement of the lung on the affected side away from the chest wall by a radiolucent band of air buy 20 gm betnovate with visa acne keloidalis nuchae surgery. The infant should be positioned so that the side of the suspected pneumothorax is up (eg buy betnovate 20 gm on-line acne nodules, if pneumothorax is suspected on the left side cheap 20gm betnovate with mastercard skin care and pregnancy, the film is taken with the left side up). It is better to treat in this setting, even if it turns out that there is no pneumothorax. There is no specific sign that distinguishes a tension from a nontension pneumothorax. Signs of a tension pneumothorax from above can also occur in a nontension pneumothorax. Just remember that in a tension pneumothorax there is an ongoing cardiopulmonary deterioration as a result of the progressive increase in intrathoracic pressure. The site of puncture should be at the second or third intercostal space along the midclavicular line. Connect a 21 or 23-gauge scalp vein needle or a 22 or 24-gauge Angiocath to a 20-mL syringe with a stopcock attached. Insert the needle above the rib, and advance it until air is withdrawn from the syringe. The needle may be removed before the chest tube is placed if the infant is relatively stable, or it may be left in place for continuous aspiration while the chest tube is being placed. If an Angiocath is used, the needle can be removed and the catheter left in place. If positive-pressure mechanical ventilation is the cause of asymptomatic pneumothorax, a chest tube will probably need to be inserted because the pressure being given by the ventilator will prevent resolution of the pneumothorax, and tension pneumothorax may develop. If a pneumothorax develops in a patient who is ready to be extubated, clinical judgment must be used in deciding whether a chest tube should be placed. If positive-pressure mechanical ventilation is not being administered, one of two treatments may be used. Close observation with follow-up chest x-ray studies every 8-12 h or sooner if the infant becomes symptomatic. For more rapid resolution of the pneumothorax in the asymptomatic patient, give the infant 100% oxygen for 8-12 h, a procedure known as nitrogen washout therapy. Less nitrogen is able to enter the lungs, and at the same time absorption of nitrogen from the extrapleural space is increased and then exhaled. The total gas tension is decreased, which also facilitates absorption of nitrogen by the blood. The method should be used only in full-term infants in whom retinopathy of prematurity will not be a problem. If respiratory failure is occurring, the treatment is usually surgical excision of the affected lobe. Positioning the infant with the affected (hyperinflated) side down may speed resolution. Pneumopericardium should be treated emergently by pericardiocentesis (see Chapter 26). Therefore, treatment should never be initiated based on heelstick Hct values alone; a central (peripheral venous stick) Hct is needed. If the sample is from the umbilical vein or radial artery, the upper limit of normal is 63%. Symptoms and signs of polycythemia include respiratory distress, tachypnea, hypoglycemia, lethargy, irritability, apnea, seizures, jitteriness, vomiting, weak sucking reflex, poor feeding, and cyanosis. Poor control of diabetes during pregnancy leads to chronic fetal hypoxia, which may result in increased neonatal erythropoiesis. Hemoconcentration secondary to dehydration is suspected if >8-10% of the birth weight has been lost. Placental transfusion occurs with delayed cord clamping, twin-twin transfusion, fetomaternal transfusion, or perinatal asphyxia. It may be seen in postmature or small for gestational age infants, preeclampsia/ eclampsia, and infants of diabetic mothers as well as with maternal use of the drug propranolol. Maternal smoking and severe maternal heart disease may also cause intrauterine hypoxia. Ruddiness, plethora, or "pink-on-blue" or "blue-on-pink" coloration may be evident. The serum glucose level should be checked because hypoglycemia is commonly seen with polycythemia. Infants with polycythemia have problems with hyperbilirubinemia because of the increased turnover of red blood cells. Serum sodium and blood urea nitrogen levels should be obtained if dehydration is being considered. One can see cardiomegaly and increased pulmonary vascular markings on a chest-x-ray. An abnormal electrocardiogram and electroencephalogram can be seen, but these tests are not routinely indicated. If the central Hct is high, either dehydration or true polycythemia is present (for treatment, see sections V,B and V,C). If the infant is dehydrated but does not have symptoms or signs of polycythemia, a trial of rehydration over 6-8 h can be attempted.
Screening may be considered in patients 216 Guidelines for Perinatal Care with a personal history of venous thromboembolism that was associated with a nonrecurrent risk factor (eg buy betnovate 20 gm line acne on buttocks, fractures buy betnovate 20 gm low cost acne at 40, surgery quality 20gm betnovate acne essential oils, and prolonged immobilization) or who have a first-degree relative with a history of high-risk thrombophilia or venous thromboembolism before age 50 years in the absence of other risk fac tors order 20 gm betnovate mastercard acne medication prescription. Testing for inherited thrombophilias in women who have experienced a recur rence of fetal loss, placental abruption, previous intrauterine growth restriction, or previous preeclampsia is not recommended. Whenever possible, laboratory testing should be performed remote (after 6 weeks) from the thrombotic event while the patient is neither pregnant nor taking anticoagulation nor hormonal therapy. Management the decision to not use pharmacologic therapy or to treat with thrombopro phylaxis or full anticoagulation is influenced by the venous thromboembolism history, severity of inherited thrombophilia, and additional risk factors. All patients with inherited thrombophilias should undergo individualized risk assessment, which may modify management decisions. As the rate of obesity increases, the number of obese women of childbearing age considering bariatric surgery also increases, which results in questions about pregnancy after these types of surgeries. It is important for obstetric care providers to counsel obese patients with specific information concerning the maternal and fetal risks of obesity in pregnancy and to address prenatal and peripartum care considerations that may be especially relevant for obese patients, including those who have undergone bariatric surgery. Obesity During pregnancy, obese women are at increased risk of several adverse perina tal outcomes, including anesthetic, perioperative, and other maternal and fetal complications. Compared with nonobese women, obese patients are at high risk of preeclampsia; gestational diabetes; preterm birth; cesarean delivery; and Obstetric and Medical Complications 217 operative and postoperative complications, including prolonged operating times and increased rates of excessive blood loss, wound infection, thromboembo lism, and endometritis. Obese women are less likely to have a successful vaginal delivery than nonobese patients, and the success rate of attempted vaginal birth after cesarean delivery is very low in extremely obese women. Maternal obesity can have deleterious effects on the fetus, including increased risks of congenital anomalies, growth abnormalities, miscarriage, and stillbirth. The most common types of obesity-associated birth defects are related to the neural tube, cardiac systems, and facial clefting, even after controlling for the diabetes. In addi tion, increased body mass impairs visualization of ultrasound images and can compromise prenatal diagnosis of fetal anomalies. Maternal obesity also may be associated with an increase risk of subsequent childhood obesity. Nutrition consultation should be offered to all obese women and they should be encouraged to follow an exercise program. This consulta tion should continue postpartum and before attempting another pregnancy. Consideration should be given to screening for gestational diabetes upon presentation or during the first trimester and repeating it later in pregnancy if the initial screening result is negative. Because these patients are at increased risk of emergent cesarean delivery and anesthetic complications, anesthesiology consultation before delivery is encouraged. Because of the increased likelihood of complicated and emergent cesarean delivery, extremely obese women may require specific resources, such as additional blood products, a large operating table, and extra personnel in the delivery room. Particular attention to the type and placement of the surgical incision is needed (ie, placing the incision above the pannicu lus adiposus). The decision to perform a primary cesarean delivery for obese women should be based on standard maternal and fetal indications. Because of the increased risk of venous thromboembolism associated with cesarean deliv ery and obesity, individual risk assessment may require additional thrombo prophylaxis with unfractionated heparin or low molecular weight heparin, in addition to the recommended use of pneumatic compression devices, during 218 Guidelines for Perinatal Care and after cesarean delivery in obese patients (see also �Deep Vein Thrombosis and Pulmonary Embolism� later in this chapter). Bariatric Surgery As the rate of obesity increases, it is becoming more common for providers of women�s health care to encounter patients who are either contemplating or have had operative procedures for weight loss, also known as bariatric surgery. The types of procedures commonly performed today include the Roux-en-Y gastric bypass (a combination of restrictive and malabsorptive effect) and adjustable gastric banding (restrictive). Researchers have determined that preg nancies after bariatric surgery are less likely to be complicated by gestational diabetes, hypertension, macrosomia, and cesarean delivery than are pregnancies of obese women who have not had the surgery. Although pregnancy outcomes generally have been favorable after bariatric surgery, nutritional and surgical complications can occur and some of these complications can result in adverse perinatal outcomes. The counseling and management of patients who become pregnant after bariatric surgery can be complex. Contraception and preconception counseling should be a component of the overall counseling for any reproductive-aged woman undergoing bariatric surgery. Contraceptive counseling is especially important for adolescents because pregnancy rates after bariatric surgery are double the rate in the general adolescent population (12. Because there is an increased risk of oral contraception failure after bariatric surgery, with a significant malabsorption component, nonoral administration of hormonal contraception should be considered in these patients. Some authorities have recommended waiting 12�24 months after bariatric surgery before conceiving so that the fetus is not exposed to a rapid maternal weight loss environment and so that the patient can achieve full weight loss goals. Should pregnancy occur before this recommended time frame, close sur veillance of maternal weight and nutritional status may be beneficial. Broad evaluation for micronutrient deficien cies (particularly, iron, vitamin B12, folate, and calcium) at the beginning of pregnancy for women who have had bariatric surgery should be considered. If there is a proven deficit, then appropriate treatment should be instituted and monitored. In the absence of a deficiency, monitoring the blood count, iron, ferritin, and calcium levels in every trimester may be considered. Alternative testing for Obstetric and Medical Complications 219 gestational diabetes should be considered for those patients with a malabsorp tive-type surgery. All gastrointestinal problems, such as nausea, vomiting, and abdominal pain, which occur commonly during pregnancy, should be thor oughly evaluated in patients who have had bariatric surgery. Early involvement of the bariatric surgeon in evaluating abdominal pain is critical because the underlying pathology may relate to the weight loss surgery. Other concerns for patients who have had bariatric surgery relate to medication dosages.
Buy generic betnovate 20 gm online. My Skin Care Regimen! - kristindaniell.com.