
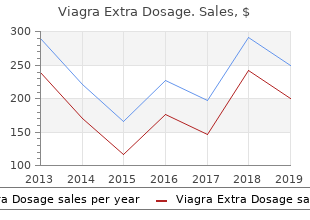
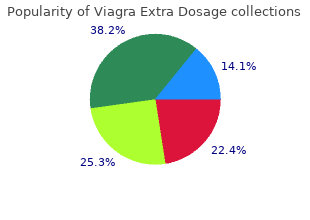
Viagra Extra Dosage
"Buy cheap viagra extra dosage 200mg on-line, impotence 21 year old."
By: William A. Weiss, MD, PhD
- Professor, Neurology UCSF Weill Institute for Neurosciences, University of California, San Francisco, San Francisco, CA

https://profiles.ucsf.edu/william.weiss
Is minocycline therapy in acne associated with antineutrophil cyto plasmic antibody positivity purchase viagra extra dosage 200mg erectile dysfunction meaning. S Clinical manifestations Pruritus Contact dermatitis Occupational asthma and rhinitis S Diagnostic methods Skin tests: none validated Positive skin prick tests in few cases Specific serum IgE: no assay commercially available Positive sIgE in few cases S Mechanisms Unknown order viagra extra dosage 130 mg amex erectile dysfunction medication canada. A therapeutic approach in the treatment of infections of the upper airways: thiamphenicol glycinate acetylcysteinate in sequential treatment (systemic-inhalatory route) order viagra extra dosage 120mg on line erectile dysfunction za. Three cases of occupational asthma induced by thiamphenicol: detection of serum-spe cific IgE buy discount viagra extra dosage 120mg online impotence with antihypertensives. Recent clinical evidence of the efficacy and safety of thiamphenicol glycinate acetylcy steinate and thiamphenicol glycinate. Molecular features determining reactivity in allergic contact dermatitis to chloramphenical and azidam phenical. Facial contact dermatitis from chloramphenicol with cross-reactivity to thiamphenicol. Preferred antimicrobial agent for the treatment of methicillin-resistant Staphylococcus aureus. Signs appear a few mns after the beginning of the injec tion or soon after the end of the infusion. It is caracterized by pruri tus, flushing, erythematous rash (face, neck and upper thorax predominantly) associated to fever, chills and in severe cases to angioedema, hypotension. One case reported with specific histamine release and cross-reactivity between vancomycin and tei coplanin. S Mechanisms �Red man syndrome� is due to histamine release into the blood by vancomycin with no antibody or complement involved. Myocardial dysfunction is secondary to endogenous myocardial histamine release, or direct inotropic myocardial depression. Pretreatment with an antihistamine (hydroxyzine 50 mg 2 hours before a vancomycin dose). IgE-mediated allergy to pyrazolones, quinolones and other non-betalactam antibiotics. Toxic epidermal necrolysis after vancomycin in a patient with terminal renal insufficiency: interest for intensive haemodialysis. Vancomycin-associated linear IgA bullous dermatosis mimicking toxic epider mal necrolysis. Successful vancomycin desensitization with a combination of rapid and slow infusion methods. Vancomycin-induced linear IgA bullous disease presenting as toxic epider mal necrolysis. In spite of the development of new antifungal drugs, amphotericin B deoxycholate remains the gold standard in the treatment of severe fungal infections in immunosuppressed hosts. S Incidence Rare allergic reactions: 3/133 patients treated with amphotericine B deoxycholate; some cases with liposomal amphotericin B. Lower nephrotoxicity with liposomal amphotericin B compared to other amphotericins. Skin tests: no evidence of specific IgE by means of prick test or intradermal test. S Management In most cases of liposomial amphotericin B reactions, switching to a different lipid formulation of amphotericin B is advised. Paradoxically, in some patients lipid formulations may be less well tole rated than conventional amphotericin B. The hepatotoxicity of antifungal medications in bone marrow transplant recipients. Amphotericin-induced stridor: a review of stridor, amphotericin preparations, and their immunoregulatory effects. S Clinical manifestations � Cutaneous: They are observed with topical use: irritating dermatitis and contact dermatitis, often unrecognized, because imputed to an increase of the initial herpes, photoallergic contact dermatitis. Systemic administration: generalized eczema, vesicular eruption, phlebitis, urticaria. S Diagnostic methods Skin tests Patch-tests with the antiviral topical drug and with detail of the constituents: acyclovir 10% in pet, propylene glycol 5 % in pet, poloxamere 407 10% in pet, cetyl stearyl alcohol 20% in pet, sodium lau ryl sulfate 1% in water. After contact dermatitis, cross reaction when systemic administration with acyclovir, valacyclovir and famciclovir. Systemic acyclovir reaction subsequent to acyclovir contact allergy: wich systemic antiviral drug should then be used. S Diagnostic methods Skin tests: none validated One case with positive skin prick tests 1/10. Patch tests with fluconazole 10% in pet applied at the site of previous lesion (fixed drug eruption). Acute generalized exanthematous pustulosis due to fluconazole (Article in French). Desensitization for fluconazole hypersensitivity J Allergy Clin Immunol 1996;98:845-6. S Diagnostic methods No in vitro or in vivo tests are available S Mecanisms Unknown. Desensitization possible for isolated generalized severe rash: beginning doses of 0. S Clinical manifestations � Cutaneous: urticaria, angioedema, purpuric drug eruption, maculopapular eruption, acute gene ralized exanthematous pustulosis, photosensitivity (rare), fixed drug reaction (rare) � Others: hepatotoxicity, serum sickness-like illness S Diagnostic methods None Skin tests: no evidence of specific IgE by means of prick test or intradermal test.
The utility of the traditional risk assessment paradigm for autoimmunity associated with environmental agents is currently limited cheap viagra extra dosage 130mg on-line erectile dysfunction prostate. A state of protection against pathogen induced injury viagra extra dosage 130 mg erectile dysfunction ear, with rapid immune elimination of pathogenic invaders; due to buy viagra extra dosage 200 mg low cost erectile dysfunction 2 previous immunization or vaccination 150mg viagra extra dosage with amex erectile dysfunction treatment in sri lanka. Adrenocortical hypofunction characterized by hypotension, weight loss, anorexia, and weakness. Autoantibodies specific to the adrenal cortex are specific diagnostic markers of this form. Interactions with each other as receptors and corres ponding ligands facilitate cooperation (cross-talk) of cells, signal transduction, and information transfer between cells. A reduction in number or mass of circulating red blood cells that may cause hypoxia in organs or tissues by the reduction in the oxygen-carrying capacity (reduction in haemoglobin concentration) of blood. Anaemia is caused either by decreased production or by increased destruction of red blood cells. Immune mediated forms of anaemia caused by decreased production of red blood cells are autoimmune myelopathies including aplastic anaemia, pure red cell aplasia induced by autoantibodies against erythropoietin, and pernicious anaemia caused by autoantibody mediated vitamin B12 deficiency (autoantibodies against gastric intrinsic factor lead to decreased absorption of vitamin B12). Lack of immune responsiveness (usually defined as lack of response to common recall antigens). The failure of B or T cells to proliferate in response to defined autoantigens (clonal anergy) is a primary mechanism of self-tolerance. An immunoglobulin produced by activated B cells and plasma cells after exposure to an antigen with specificity for the inducing antigen. Lysis of various target cells coated with antibody by Fc receptor bearing killer cells, including large granular lymphocytes (natural killer cells), neutrophils, eosinophils, and mononuclear phago cytes. Antigens inducing immune responses only with the help of T cells are T cell-dependent antigens, while those that do not need T cell help are T cell-independent antigens. Epitopes are recognized by antigen receptors on T or B cells (T cell epitopes or B cell epitopes). Non-organ-specific autoanti bodies directed against various nuclear antigens, including chro matin antigens. Autoantibodies directed against neutral or negatively charged phospholipids including anticardiolipin antibodies (aCl) and lupus anticoagulant. They are diagnostic markers of the antiphospholipid syndrome, although they are also found in patients with other (autoimmune) diseases and infections. Programmed cell death, a physiological process whereby useless and potentially harmful cells are rapidly eliminated without tissue inflammation or damage. See also: Fas and Fas ligand, autoimmune lymphoproliferative syndrome, Bcl-2. It is a multifactorial process leading to the accumulation of lipids within the vessel wall, associated with mononuclear cell infiltration and smooth muscle proliferation. Autoimmune-mediated inflammation may play an important role in accelerated atherosclerosis in autoimmune rheumatic diseases. They circulate in the serum but may also be detectable in other body fluids or bound in target tissue structures. Self-antigens of the organism, which may be targets of autoimmune responses by autoreactive B cells (see: autoantibodies) or T cells, including proteins. Autoimmune haemolytic anaemia may be idiopathic, secondary to lymphoproliferative, auto immune. See also: anaemia, cold autoantibody type, warm autoantibody type, drug-induced immune haemolytic anaemia. Associated with defects in the Fas�FasL apoptosis signalling pathway due to mutations in the Fas gene, the FasL gene, or other genes coding for factors of this pathway. Destructive autoimmunity is associated with the development of autoimmune diseases. Human oncoprotein that plays a role in tissue develop ment and maintenance by preventing apoptosis of specific cell types. Bone marrow-derived lymphocytes, expressing an antigen�receptor complex composed of membrane bound immunoglobulin (mIg) and associated molecular chains. May be idiopathic or paraneoplastic (caused by various lymphoproliferative malignancies). Seems to be important in preventing the development of autoimmune diseases (depletion leads to the spontaneous development of various autoimmune diseases in genetically susceptible animals; transfer prevents the development of organ-specific autoimmunity). In rheumatoid arthritis, these cells can account for up to 60% of circulating B cells and may produce rheumatoid factor. Functional alterations were shown to be associated with the relapse of auto immune diseases. A specific immune response in which T lymphocytes mediate the effects, either through the release of cytokines or through cytotoxicity. Large family of small secreted proteins (8�15 kilodaltons) that control the trafficking of leukocyte subpopulations, induce leukocyte activation, and control lymphocyte differen tiation and effector function. May play an important role in the pathogenesis of autoimmune diseases, because the migration and accumulation of leukocytes in the target organs are critical steps for this. Failure of B or T cells expressing anti-self-receptors to interact with antigen. As an effector mechanism of the humoral immune response, the activated com plement system facilitates opsonization, phagocytosis, and lysis of cellular antigens. Systemic autoimmune rheumatic diseases, including systemic lupus erythematosus, Sjogren syn drome, systemic sclerosis (scleroderma), autoimmune myositis (polymyositis, dermatomyositis), mixed connective tissue disease, and other overlapping syndromes.
Intrahepatic porto-systemic Serum antimitochondrial buy viagra extra dosage 120mg without prescription erectile dysfunction under 25, antinuclear buy viagra extra dosage 120mg without a prescription erectile dysfunction 20s, anti smooth muscle 150mg viagra extra dosage low testosterone causes erectile dysfunction, shunts are rare generic viagra extra dosage 120mg visa impotence 19 year old. These comprise small portal veins along perinuclear antineutrophil cytoplasmic, and anti liver-kidney J Gastrointestin Liver Dis microsome antibodies were absent. The spleen was A large splenorenal collateral should be interrupted enlarged (170 x 60 mm), and splenic vein, 5 mm in diameter, during liver transplantation to secure adequate portal showed phasic flow 20 cm/sec. Ultrasonography found Percutaneous liver biopsy was performed using hydronephrosis of the left kidney, secondary to pelviureteric Menghini needle of 1. The splenic vein was prominent, with of the liver tissue confirmed chronic hepatitis, with mild a large splenic collateral coursing towards the diaphragm, activity in the stage of cirrhosis. Left renal vein catheterization was performed, effects or chronic porto-systemic encephalopathy, refractory and dilation due to splenorenal shunt was found. Venous blood is diverted from the high pressure portal only of the proximal splenic vein, leaving the shunt intact. References Doppler ultrasonography and angiography identify patients with collaterals, giving accurate mapping of porto 1. The treatment of portal systemic collaterals and avoiding complications of hypertension: natural history and prognostic factors. Intrahepatic with spontaneous porto-systemic shunts in 38%, most often portosystemic venous shunt: diagnosis by color Doppler as splenorenal shunts (21%) and patent umbilical veins imaging. The value of Doppler ultrasound in cirrhosis and varices, collaterals to thrombotic portal veins, mesoiliac portal hypertension. Scand J Gastroenterol Suppl 1999; 230: shunts, and portorenal shunts to the right kidney (7). La Villa G, Barletta G, Pantaleo P, Del Bene R, Vizzutti F, common spontaneous collateral pathway, after splenorenal Vecchiarino S. J Diagn Med with a high risk of variceal hemorrhage and associated 30 Sonography 2001; 17:193-200. Color Doppler Iannello et al described a 70-year old woman with liver sonographic evaluation of spontaneous portosystemic shunts cirrhosis secondary to chronic hepatitis B and C, and inversion of portal venous flow in patients with cirrhosis. Relationship between portal pressure response vein, but without gastroesophageal varices on endoscopic to pharmacotherapy and risk of recurrent variceal hemorrhage examination (9). Current concepts in the splenorenal shunt in a patient with liver cirrhosis and pathophysiology of hepatic encephalopathy. Living-related liver trans retrograde transvenous obliteration with ethanolamine-oleate plantation with renoportal anastomosis for a patient with large for the treatment of hepatic encephalopathy in a cirrhotic spontaneous splenorenal collateral. Indian J Gastro blood flow separation in a patient with portosystemic entrol 2004; 23:187-188. Clinical Definitions-continued � Liver failure-Failure of the liver to perform its biosynthetic functions. Abnormal Liver Tests � True liver function tests are not widely used � galactose clearance, aminopyrine clearance tests. Suggestions are: �Although nonspecfic, consider alcohol �Review risk factors for non-alcoholic fatty liver disease. Medical Director, Liver Transplant Associate Chief, Section of Hepatology Loyola University Medical Center jahn2@lumc. The liver is first visible in a developing embryo during the fourth week of preg nancy. As the fetus develops, the liver divides into two sections, called the right and left lobes. If you feel the right lower edge just under your rib cage, you may detect a firm mass that makes a solid sound when you give it a good tap. The liver, tucked under the diaphragm and ribs, extends across to the left side of the body over the top edge of the stomach. The liver�s blood supply is unique; it comes from both the heart and the digestive tract directly through a large blood vessel called the portal vein. Most livers have 50,000 to 100,000 lobules that consist of a vein surrounded by tiny liver cells, called hepatocytes. Liver cells produce proteins and lipids or fatty substances that include triglycerides, cholesterol and lipoproteins. These bile acids are neces sary for the body to absorb vitamins A, D and E, all of which are found in fat. It removes chemicals, alcohol, toxins and medicine from the bloodstream and sends them to the kidneys as urea to be excreted as urine or to the intestines to be excreted as stool. How the Liver Works When food is eaten, the nutrients travel down the throat, into the stomach and then on to the intestines. These organs break up and dissolve the food into small pieces that can be absorbed into the bloodstream. Most of these small particles travel from the intestines to the liver, which filters and converts the food into nourishment that the bloodstream delivers to cells that need it. The liver stores this nourishment and releases it throughout the day, as the body needs it. The proteins, fats, enzymes and other chemicals the liver creates from nutrients are critical to a person�s health. For instance, the liver produces the proteins that are necessary for blood to clot. When the liver cannot produce these clotting components, a person could bleed to death.
Nevertheless buy 200mg viagra extra dosage mastercard erectile dysfunction treatment injection therapy, challenge often allows figures such as positive and negative predictive value to order viagra extra dosage 150 mg overnight delivery erectile dysfunction onset be calculated buy viagra extra dosage 120mg erectile dysfunction 43 years old. The positive predictive value is the probability that a positive test represents a true allergy order viagra extra dosage 200 mg on-line impotence zargan. Many studies are emerging which attempt to determine the extent to which a particular wheal diameter can predict the risk of clinical reaction on challenge with a food. These studies have been used to suggest that challenge testing (in the case of suspected food allergy) 29 may not be necessary to confirm the diagnosis when the wheal reaches a certain diameter. However it is crucial to recognise that the likelihood of true allergy for any given skin test size will depend on the pre-test probability that the study subject has the allergy. For example the pre-test probability of peanut allergy is different in a child with a history of urticaria after eating nuts compared with a child who has eczema but no history of nut ingestion, in whom the test is performed for screening purposes. Therefore the predictive value varies in individuals with different histories, and may vary in hospital, specialist or general practice populations. A more useful figure is the likelihood ratio, which is a reflection of the degree to which the test result changes the probability that the patient has the allergy. These factors need to be taken into account not only in evaluating published studies but in applying the results of diagnostic testing to individual patients. We should note that the importance of optimal interpretation of skin prick test results depends on the allergic condition in question and the allergen being tested. For example the erroneous interpretation of skin test results for aeroallergens in a patient with allergic rhinitis might result in inappropriate allergen avoidance strategies, which may be inconvenient, but erroneous interpretation of food allergy tests can have much more serious consequences such as inappropriate dietary restrictions which might be deleterious to health, or inappropriate exposure to foods which might be dangerous. Therefore, taken together with the fact that skin testing for food is inherently more difficult to interpret, we suggest that it should be restricted to specialist practitioners. When immunotherapy for inhalant allergens is being considered, the correct interpretation of skin prick test results becomes more critical since misdiagnosis may lead to inappropriate treatment, and again it should be carried out by specialists in these circumstances. Interpretation of skin test results should be carried out by an experienced practitioner who is familiar with all of these factors. Challenge testing is also used in the research context with the specific purpose of validating the results of diagnostic tests. Challenge tests can be done by respiratory exposure (nasal or bronchial challenges) or using eyedrops of allergen solution (ocular challenge), generally with graded concentrations. Challenge testing, particularly for food and drugs, may carry significant risk and must be done with full informed consent, under close observation and monitoring, in a setting where all safety measures have been taken and equipment is readily available to treat any reactions including anaphylaxis. The location of challenge (outpatient or hospital setting) will be dependent on pre-challenge assessment of the likelihood of reaction, potential reaction severity, co-morbid conditions (such as asthma or cardiovascular disease) and facilities available to treat allergic reactions if they do occur. Personnel Skin prick testing is routinely carried out (when indicated) by allergy specialists, where it is considered an extension of the physical examination. It may also carried out by some general practitioners and other specialists (paediatricians, general physicians, thoracic physicians) who have additional training in allergy or where there are few allergy specialists available. However there is currently no certification or accreditation for performance of this test. Skin prick testing is also carried out in some respiratory laboratories and pathology laboratories; the standards in Appendix A should also apply in these settings. The evidence base for effectiveness or otherwise of allergen avoidance measures and immunotherapy must be taken into account when advising patients on management based on allergy test results. Medical practitioners involved in allergy testing should maintain a good knowledge of allergic diseases, of allergens relevant in their area, and the significance of particular skin prick test reactions in relation to the condition in question (an example might be the relative importance of allergy to dust mite, animals, pollens and foods in a case of atopic dermatitis). Role of nurses or technicians in skin prick testing: Counsel the patient prior to the test on what to expect, put them at ease, position the patient appropriately and comfortably. There is no formal training for other specialists or general practitioners who conduct allergy testing. Allergy seminars and allergy testing workshops have been run from time to time by specialist units. It is suggested that at least 10 skin tests over several days on a variety of patients should be carried out under supervision of an experienced nurse and allergy specialist to ensure basic competency. Rarely, adverse events can occur; these can be classified into allergic, test-related non allergic, and nonspecific. Examples of test-related non-allergic might include transmission of infection (theoretical but never documented); examples of nonspecific are syncope, headache etc. Vasovagal syncope is relatively common and if the test is done on the patient in the sitting position, facilities should be available for the patient to lie down if feeling faint. Delayed local skin swelling (the late phase response) which is often tender or painful may occur uncommonly as a result of an IgE-mediated late-phase reaction (seen more commonly with intradermal testing). Rarely this can cause quite marked swelling and discomfort, however it does not usually last more than 36 hours. Systemic introduction of allergen may occur as an unintended consequence of the skin prick. Systemic reactions from skin prick testing have been recorded, including the typical manifestations of anaphylaxis such as generalised urticaria, angioedema including airway angioedema, bronchospasm, and hypotension. These reactions are generally mild and respond to treatment with standard measures. There are many case reports of systemic allergic 30 reactions from prick testing (Liccardi 2006) although in large case series this is exceedingly rare. In a survey of 16,000 individuals tested with eight routine allergens, the rate of adverse 31 reactions was 0.
Which of the following is the most likely cause of urinary symptoms in this patient buy viagra extra dosage 200 mg amex prostate cancer erectile dysfunction statistics. In addition to buy discount viagra extra dosage 150mg online erectile dysfunction what is it cigarette smoking generic viagra extra dosage 150mg visa erectile dysfunction treatment orlando, which of the following (D) Malakoplakia is the most signi cant risk factor for the development of this (E) Malignant lymphoma patient�s malignant neoplasm cheap 200mg viagra extra dosage amex best erectile dysfunction pills review. Cystoscopy reveals a solitary, 2-cm papillary tumor in the posterior bladder wall. This (D) Spermatocele benign lesion is caused by infection with which of the following (E) Varicocele pathogens. Which of the following is the most likely histologic diagnosis for this malignant neoplasm. Physical examination shows suppurative (D) Liposarcoma urethritis, with redness and swelling at the urethral meatus. Biopsy of the affected tissue shows chronic in am (C) Haemophilus ducreyi mation, granulation tissue, and epithelial hyperplasia. Which of the following is the most (D) Urothelial cell papilloma likely complication of chronic balanitis in this patient. The patient�s past medical history is signi cant (D) Hypospadias for chronic schistosomiasis, which is endemic in his country (E) Phimosis of origin. Urinalysis shows malignant cells and cystoscopy reveals a mass in the wall of the urinary bladder. Which of the 19 A 65-year-old man presents with multiple lesions on his penis following is the most likely diagnosis. Physical examination reveals (A) Adenocarcinoma shiny, soft, erythematous plaques on the glans and foreskin. The Lower Urinary Tract and Male Reproductive System 201 (A) Adenocarcinoma 23 A 20-year-old intersex woman presents with questions regard (B) Lichen planus ing her sexual differentiation. Physical examination reveals (C) Melanoma ambiguous female external genital organs with signs of viril (D) Squamous cell carcinoma ization. He (A) Congenital adrenal hyperplasia could not completely empty his bladder and felt �distended� (B) Cryptorchidism and �irritated� all the time. Rectal digital examination reveals (C) Klinefelter syndrome an enlarged nodular prostate. A biopsy discloses hyperplastic (D) Testicular feminization syndrome prostatic glands (shown in the image). If this patient�s pros (E) Turner syndrome tate continues to enlarge, which of the following is a possible complication. Physical exami nation reveals a solid mass that cannot be transilluminated, and biopsy shows a haphazard arrangement of benign differ entiated tissues, including squamous epithelium, glandular epithelium, cartilage, and neural tissue. The left testicle was removed surgically, and the patient is symptom free 5 years later. Microscopic examination of the surgical specimen shows neoplastic cells forming glomeruloid Schiller-Duval (A) Adenocarcinoma of prostate bodies. Which of the following serum markers is most useful (B) Hydroureter and hydronephrosis for monitoring the recurrence of tumor in this patient. Physical examination reveals 26 A 32-year-old man presents with a testicular mass that he rst a small, tender nodule attached to the testis. An orchiec tomy is performed, and the surgical specimen is shown in the (B) Orchitis image. Laboratory studies previously identi ed a 21-hydroxylase de ciency and adrenogenital syndrome. The mass cannot be transilluminated (A) Choriocarcinoma and appears to be solid on ultrasound examination. The multinucleated giant (C) Leydig cell tumor cells in this neoplasm are derived from which of the following (D) Malignant lymphoma cell types. Physical examination reveals enlargement of the external male genitalia and facial hair. Which of the following neoplasms is the most likely cause of precocious puberty in this patient. What is the probable (A) Anorchia cause of bladder outlet obstruction in this patient. The Lower Urinary Tract and Male Reproductive System 203 Which of the following best describes the putative precursor (A) Cystitis cystica of this malignant neoplasm. Cystoscopy 37 A 55-year-old man presents with urinary symptoms of urgency reveals a mass in the dome of the bladder. Rectal examination reveals an enlarged pros cells arranged as gland-like structures. Histologic examination reveals lymphocytes and mast cells, as well as extensive bro 38 A 70-year-old man presents with pain in his back. Which of the clinical ndings include a rock-hard, enlarged prostate pal following is the most likely diagnosis. Radiologic studies show multi centric, osteoblastic lesions of the lumbar vertebral bodies. The patient is treated with leuprolide acetate (lupron), an inhibitor of gonadotropin release by the pituitary. Which of the following statements best summarizes the rationale for this treatment. Histologic examina tion shows mucosal chronic in ammatory cells with numer ous macrophages (shown in the image). The arrow (see inset) identi es small intracytoplasmic, calcium-rich spherical struc tures (Michaelis-Gutmann bodies). The affected area can be transilluminated and is 1 the answer is C: Exstrophy of urinary bladder. Microscopic examination of the bladder is a serious developmental abnormality char of the aspirated uid reveals degenerating spermatozoa.
130mg viagra extra dosage fast delivery. Get Instant Rock Hard Erections By Using 1 Minute Trick || Cure Erectile Dysfunction Naturally.