
Donepezil
"Cheap donepezil 5 mg mastercard, medications ranitidine."
By: William A. Weiss, MD, PhD
- Professor, Neurology UCSF Weill Institute for Neurosciences, University of California, San Francisco, San Francisco, CA

https://profiles.ucsf.edu/william.weiss
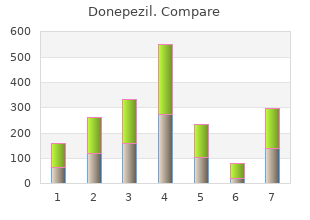
Remote Control the Remote Control will prompt you to buy donepezil 10 mg otc medicine lake montana clear the programs on the External Trial Stimulator safe 10mg donepezil medications like abilify. External Trial Stimulator the Remote Control will ask if you want to generic 5 mg donepezil fast delivery medications prescribed for pain are termed download the Remote Control Remote Control programs to best 5mg donepezil red carpet treatment the External Trial Stimulator. External Trial Enter the password A-B-C to download the Remote Control Stimulator programs to the External Trial Stimulator. Remote Control the Remote Control will be linked to the External Trial Stimulator immediately. Note: To re-link the Remote Control, see Linking a Remote Control to a Stimulator on page 4. To access the Start Screen at any other time, click from the top right corner of any screen. The toolbar allows you to access various features defined in the table below and further described in several sections of this guide. Click to Create reports, including patient information reports, generic reports, patient list reports, clinical outcomes reports, and clinic activity reports. Synchronize data between the Clinician Programmer and a Patient Card (for data transfer). These buttons allow you to quickly and conveniently access common screens or perform common actions. The function of these buttons are defined in the table below and further described in several sections of this guide. Turn stimulation on (applies to all areas with Amplitude set at a value greater than zero). When the software is already open, you may start a new session or restart the Bionic Navigator software using the Start function. For more information on the Profile Screen, see Managing a Patient�s Profile on page 13. To select an existing patient: 1 Click the down arrow on the right side of the Patient pull-down menu. You may now proceed to other screens by clicking the appropriate buttons on the screen. If a patient is currently selected, the patient�s information will show up on the Profile Screen. Note: If no patient was selected, it is assumed that you wish to create a new patient and the fields on the Profile Screen will be empty. Note: In the event that any button other than is selected, the patient information entered will automatically be saved. The information entered is stored and can be chronologically viewed in the patient�s case history. To enter notes: 1 If you are not currently in the Profile Screen, click in the upper right corner of any screen. Current notes are editable, but past notes are read-only and can be viewed in the case history. Each visit is time stamped and displayed along with the Reason for Visit and Notes. Note: Patient visits are recorded and time stamped only when the user exits or saves the Profile Screen. To view a patient�s Case History: 1 If you are not currently in the Profile Screen, click in the upper right corner of any screen. The Stimulator and Remote Control product and serial numbers are automatically detected and recorded. If Lead information has not been entered, the information will be requested before the Configuration screen is displayed. By default, Bionic Navigator assigns contacts 1-8 to the left Lead and contacts 9-16 to the right Lead. To aid in programming the Stimulator, you may wish to rearrange the display so that the Lead connected to port 1-L (contacts 1-8) appears on the right, and the Lead connected to port 2-R (contacts 9-16) appears on the left. Note: this function only visually changes the order of the Leads on the Configuration and Programming screens. It does not change the order of the Leads displayed in reports or programs, which list contacts 1-8 followed by contacts 9-16. To rearrange the display of the Lead(s) (left to right): 1 Click from the Configuration screen. Lead impedance is measured and displayed for each of the Stimulator�s 16 contacts. Impedances over 4500 are considered to be resultant from open or unconnected wires and are displayed with an orange bar on the Impedance screen (or an �X� on the Program screen). To check the Lead impedances: 1 Click while in the Configuration screen or the Program screen. It is also possible to configure a single lead with both monopolar and multipolar areas, as long as the same contacts are not used in both. The above graph shows the maximum output current when stimulation settings are set to the maximum values on an electrode (Amplitude Max = 12. For example, one Area may correspond to a right brain target, while another Area may correspond to a left brain target. These Areas run in an interleaved fashion, and multiple Areas (up to four) constitute a program. Stimulation parameters and the contact configuration are displayed for one selected Area at a time. To select an Area: 1 Click the on the desired Area control box on the left of the Programming screen, as highlighted in the image below.
Acute interventions can be envisioned as the mental health correlate of physical first aid purchase donepezil 10 mg without prescription medications covered by medi cal, with the goal being to buy donepezil 10 mg visa symptoms zyrtec overdose �stop the psychological bleeding purchase 10mg donepezil overnight delivery xanax medications for anxiety. Once the patient is in a safe situation buy donepezil 5 mg line symptoms 5 days before your missed period, the provider should attempt to reassure the patient, encourage a professional healing relationship, encourage a feeling of safety, and identify existing social supports. Establishing safety and assurance may enable people to get back on track, and maintain their pre-trauma stable condition. Address acute medical/behavioral issues to preserve life and avoid further harm by: a. Arrange a safe, private, and comfortable environment for continuation of the evaluation: a. Maintain a supportive, non-blaming, non-judgmental stance throughout the evaluation d. Assist with the removal of any ongoing exposure to stimuli associated with the traumatic event. Evacuate to next level of care if unmanageable, if existing resources are unavailable, or if reaction is outside of the scope of expertise of the care provider. Risk factors for suicide should also be assessed, such as current depression and substance abuse. If significant suicidality is present, it must be addressed before any other treatment is initiated. Some individuals with stress reactions could be at risk for violence toward others. This can be manifested through explosivity and anger problems and may predict risk for violent behavior. For extended discussion of dangerousness to self or others, see Module B: Annotation C � Assessment of Dangerousness. Their normal shelter, clothing, and other basic resources may be destroyed or inaccessible. Early interventions should typically seek to address the needs of the individual person, with the aim of promoting normal recovery, resiliency, and personal growth and avoiding additional harm (see Table A-1 Early Interventions. Individual persons who were exposed to trauma as members of a group/unit that existed prior to the trauma event. Some of the acute interventions, such as psychoeducation, may be provided in a group format to maintain unit integrity and promote continuity with established relationships. If indicated, reduce use of alcohol, tobacco, caffeine, and illicit psychoactive substances. Assign job tasks and recreational activities that will restore focus and confidence and reinforce teamwork (limited duty). When the patient is in a safe situation, the clinician should attempt to reassure the patient and encourage a feeling of safety. The fewer traumatic stimuli people see, hear, smell, taste, or feel, the better off they will be. When possible, direct ambulatory survivors: o Away from the site of destruction o Away from severely injured survivors o Away from continuing danger. Connect: Survivors who are encountered will usually have lost connection to the world that was familiar to them. A supportive, compassionate, and nonjudgmental verbal or nonverbal exchange between you and survivors may help to give the experience of connection to the shared societal values of altruism and goodness. Help survivors connect: o To loved ones o To accurate information and appropriate resources o To locations where they will be able to receive additional support o To unit comrades and mission, fostering vertical and horizontal cohesion. However, some may require immediate crisis intervention to help manage intense feelings of panic or grief. It is included as part of the Fundamental Criteria for First Aid knowledge and skills that soldiers should be trained in order to save themselves or other soldiers in casualty situations. Contact and Engagement Respond to contacts initiated by affected persons, or initiate contacts in a non-intrusive, compassionate, and helpful manner 2. Safety and Comfort Enhance immediate and ongoing safety, and provide physical and emotional comfort 3. Stabilization (if needed) Calm and orient emotionally overwhelmed or distraught survivors 4. Practical Assistance Offer practical help to the survivor in addressing immediate needs and concerns 6. Connection with Social Supports Help establish opportunities for brief or ongoing contacts with primary support persons or other sources of support, including family members, friends, and community helping resources 7. Information on Coping Provide information (about stress reactions and coping) to reduce distress and promote adaptive functioning 8. Linkage to Collaborative Services Link survivors with needed services and inform them about available services that may be needed in the future. The amount of time spent on each goal will vary from person to person and with different circumstances, according to need. Stress is inevitable in combat, in hostage and terrorist situations, and in civilian disasters, such as floods, hurricanes, tornadoes, and industrial and aircraft catastrophes. Most emotional reactions to such situations are temporary, and the person can still carry on with encouragement. However, if the stress symptoms are seriously disabling, they may be psychologically contagious and endanger not only the emotionally upset individual but also the entire unit. Even when there is no immediate danger of physical injury, psychological harm may occur. Emotional distress is not always as visible as a wound, a broken leg, or a reaction to pain from physical damage. However, overexcitement, severe fear, excessive worry, deep depression, misdirected aggression, or irritability and anger are signs that stress has reached the point of interfering with effective coping. The discovery of a physical injury or cause for an inability to function does not rule out the possibility of a psychological injury (or vice versa).
Donepezil 10mg otc. Strep Throat Symptoms - wikiSymptoms.
Comparison of pain and emotional symptoms in soldiers with polytrauma: unique aspects of blast exposure cheap donepezil 5mg overnight delivery symptoms vertigo. The impact of borderline personality disorder on process group outcome among women with posttraumatic stress disorder related to generic donepezil 10 mg with visa medications grapefruit interacts with childhood abuse discount donepezil 10 mg visa medicine in the 1800s. Repetitive transcranial magnetic stimulation of the right dorsolateral prefrontal cortex in posttraumatic stress disorder: a double-blind donepezil 10 mg with amex medications without doctors prescription, placebo-controlled study. Social support protects against the negative effects of partner violence on mental health. Integrating complementary therapies into community mental health practice: an exploration. Tiagabine for posttraumatic stress disorder: effects of open-label and double-blind discontinuation treatment. Dissemination and feasibility of a cognitive behavioral treatment for substance use disorders and posttraumatic stress disorder in the Veterans Administration. Randomized controlled comparison of cognitive behavior therapy with rogerian supportive therapy in chronic post-traumatic stress disorder: A 2-year follow-up. A pilot controlled study of the effects of flumazenil in posttraumatic stress disorder. Creamer M, Parslow R: Trauma exposure and posttraumatic stress disorder in the elderly: a community prevalence study. Population-based norms for the Mini-Mental State Examination by age and educational level. Preventing the incidence of new cases of mental disorders: a meta analytic review. Public service reductions associated with placement of homeless persons with severe mental illness in supportive housing. Efficacy of sertraline in preventing relapse of posttraumatic stress disorder: results of a 28-week double-blind, placebo-controlled study. Venlafaxine extended release in posttraumatic stress disorder: a sertraline and placebo-controlled study. The Efficacy and Tolerability of Tiagabine in Adult Patients With Post-Traumatic Stress Disorder. Maintenance therapy with fluoxetine in posttraumatic stress disorder: a placebo-controlled discontinuation study. Multicenter, double-blind comparison of sertraline and placebo in the treatment of posttraumatic stress disorder. Divalproex in the treatment of posttraumatic stress disorder: a randomized, double-blind, placebo-controlled trial in a veteran population. A placebo-controlled study of nefazodone for the treatment of chronic posttraumatic stress disorder: a preliminary study. A placebo-controlled trial of guanfacine for the treatment of posttraumatic stress disorder in veterans. Posttraumatic stress disorder in general intensive care unit survivors: a systematic review. Evaluation of physical activity habits in patients with posttraumatic stress disorder. The lifetime prevalence of traumatic events and posttraumatic stress disorder in the Netherlands. Some implications of former massive traumatization upon the actual analytic process. Preventing psychological trauma in soldiers: the role of operational stress training and psychological debriefing. The effects of an aerobic exercise program on posttraumatic stress disorder symptom severity in adolescents. Meta-analytic evaluation of skills training research for individuals with severe mental illness. Similarity of prior trauma exposure as a determinant of chronic stress responding to an airline disaster. Antidepressant treatment of posttraumatic stress disorder and major depression in veterans. The New Hampshire study of supported employment for people with severe mental illness. The impact of enhanced incentives on vocational rehabilitation outcomes for dually diagnosed veterans. Adding contingency management intervention to vocational rehabilitation: outcomes for dually diagnosed veterans. Efficacy of buspirone in the treatment of posttraumatic stress disorder: an open trial. Post-traumatic stress disorder in the context of terrorism and other civil conflict in Northern Ireland: Randomised controlled trial. Risk factors for clinically recognized opioid abuse and dependence among veterans using opioids for chronic non-cancer pain. A randomized controlled trial of cognitive therapy, a self-help booklet, and repeated assessments as early interventions for posttraumatic stress disorder. Hypnotic change in combat dreams of two veterans with posttraumatic stress disorder. The effects of group psychological debriefing on acute stress reactions following a traffic accident: a quasi-experimental approach. Relationship of physical symptoms to posttraumatic stress disorder among veterans seeking care for Gulf War-related health concerns.
The Examiner should inquire about the place order donepezil 10 mg fast delivery medications high blood pressure, cause donepezil 5mg for sale medications quotes, and date of rejection and enter the information in Item 60 buy cheap donepezil 10mg on line symptoms 0f heart attack. It is helpful if the Examiner can assist the applicant with obtaining relevant military documents buy donepezil 5mg without prescription treatment 4 toilet infection. For each admission, the applicant should list the dates, diagnoses, duration, treatment, name of the attending physician, and complete address of the hospital or clinic. The applicant must name the charge for which convicted and the date of the conviction(s), and copies of court documents (if available). If additional records, tests, or specialty reports are necessary in order to make a certification decision, the applicant should so be advised. If the applicant does not wish to provide the information requested by the Examiner, the Examiner should defer issuance. The applicant must report any disability benefits received, regardless of source or amount. The Examiner must document the specifics and nature of the disability in findings in Item 60. Visits to Health Professional Within Last 3 Years the applicant should list all visits in the last 3 years to a physician, physician assistant, nurse practitioner, psychologist, clinical social worker, or substance abuse specialist for treatment, examination, or medical/mental evaluation. The applicant should list visits for counseling only if related to a personal substance abuse or psychiatric condition. The applicant should give the name, date, address, and type of health professional consulted and briefly state the reason for the consultation. Multiple visits to one health professional for the same condition may be aggregated on one line. When an applicant does provide history in Item 19, the Examiner should review the matter with the applicant. The Examiner will record in Item 60 only that information needed to document the review and provide the basis for a certification decision. If the Examiner finds the information to be of a personal or sensitive nature with no relevancy to flying safety, it should be recorded in Item 60 as follows: 36 Guide for Aviation Medical Examiners "Item 19. The Examiner must list the facts, such as dates, frequency, and severity of occurrence. Although there are no medical standards for height, exceptionally short individuals may not be able to effectively reach all flight controls and must fly specially modified aircraft. If the Examiner finds the condition has become worse, a medical certificate should not be issued even if the applicant is otherwise qualified. The head and neck should be examined to determine the presence of any significant defects such as: a. The external ear is seldom a major problem in the medical certification of applicants. Discharge or granulation tissue may be the only observable indication of perforation. Mobility should be demonstrated by watching the drum through the otoscope during a valsalva maneuver. Pathology of the middle ear may be demonstrated by changes in the appearance and mobility of the tympanic membrane. An upper respiratory infection greatly increases the risk of aerotitis media with pain, deafness, tinnitus, and vertigo due to lessened aeration of the middle ear from eustachian tube dysfunction. If the condition is not a threat to aviation safety, the treatment consists solely of antibiotics, and the antibiotics have been taken over a sufficient period to rule out the likelihood of adverse side effects, the Examiner may make the certification decision. The same approach should be taken when considering the significance of prior surgery such as myringotomy, mastoidectomy, or tympanoplasty. An applicant with unilateral congenital or acquired deafness should not be denied medical certification if able to pass any of the tests of hearing acuity. It is possible for a totally deaf person to qualify for a private pilot certificate. The student may practice with an instructor before undergoing a pilot check ride for the private pilot�s license. If the applicant is unable to pass any of the above tests without the use of hearing aids, he or she may be tested using hearing aids. The nose should be examined for the presence of polyps, blood, or signs of infection, allergy, or substance abuse. The Examiner should determine if there is a history of epistaxis with exposure to high altitudes and if there is any indication of loss of sense of smell (anosmia). Anosmia is at least noteworthy in that the airman should be made fully aware of the significance of the handicap in flying (inability to receive early warning of gas spills, oil leaks, or smoke). Evidence of sinus disease must be carefully evaluated by a specialist because of the risk of sudden and severe incapacitation from barotrauma. The mouth and throat should be examined to determine the presence of active disease that is progressive or may interfere with voice communications. Gross abnormalities that could interfere with the use of personal equipment such as oxygen equipment should be identified. Any applicant seeking certification for the first time with a functioning tracheostomy, following laryngectomy, or who uses an artificial voice-producing device should be denied or deferred and carefully assessed. The worksheets provide detailed instructions to the examiner and outline condition-specific requirements for the applicant. For example, if the medication is taken every 4-6 hours, wait 30 hours (5x6) after the last dose to fly. Some conditions may have several possible causes or exhibit multiple symptomatology. Transient processes, such as those associated with acute labyrinthitis or benign positional vertigo may not disqualify an applicant when fully recovered.