
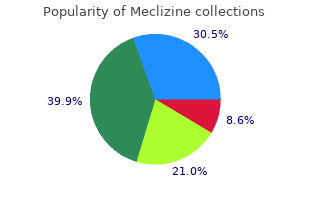
Meclizine
"Buy discount meclizine 25mg on line, medicine mountain scout ranch."
By: Bertram G. Katzung MD, PhD
- Professor Emeritus, Department of Cellular & Molecular Pharmacology, University of California, San Francisco
http://cmp.ucsf.edu/faculty/bertram-katzung
The complications of family relationships in surrogacy are such that the child will have to order 25mg meclizine visa symptoms zyrtec overdose be told about their conception and birth buy meclizine 25mg with mastercard medications versed. In most countries the adoption and parental change arrangements will mean that the child has the right to discount meclizine 25 mg without prescription treatment zamrud their original birth certificate on reaching 18 years of age generic meclizine 25mg aquapel glass treatment. Legal knowledge is necessary because there will be procedures which may involve adoption after the birth of the child. In many cases successful parents are so delighted with the outcome that they may forget what those procedures are and they may well need further contact with the counsellor to remind themselves of the proper steps forward. Counsellors may need a couple�s permission to divulge to the courts the fact that they were counselled. Good information in the form of booklets often provides a reference which parent can refer to at a later stage. There should be the opportunity for good follow up counselling and an awareness for all the parties concerned that further counselling support will be available for commissioning couples, the children and the-surrogates for as long as they may need it. Counsellors must be aware themselves of their role in surrogacy and be clear that the couples understand that role. Treatment by in vitro fertilisation with surrogacy: experience of one British Centre. However this relation ship with the child may not be an exclusive one because in some European countries there are systems of open adoption where the natural parents still have rights of access to their child. For example in the United Kingdom an adoption order will transfer all legal rights of parenthood to adoptive parents including inheritance but the natural parents may have rights of contact by letter or in person. Obviously this would not satisfy those people for example, searching for a tight nuclear family or a close exclusive relationship with their child. Adoption is also available to those who are not infertile and who have no medical problems; this means that any person with infertility problems has competition and faces additional assessment for the smaller number of children requiring a permanent home. Such applicants are at further disadvantage as they may not be able to demonstrate successful parenting skills. These are particularly important as the children available nowadays are likely to be older or have special needs. Prior to the 1980�s adoption, along with surrogacy and artificial insemination with donor or husband sperm were the major route to achieving parenthood for those with infertility problems. Since that time, scientific advance in the field of reproduction, along with changing social atti tudes and greater state support for parents, has meant that those people who would previously have placed a child for adoption now keep the child instead. Thus adoption is no longer an easily available route to parenthood for most people in Europe. Some choose to adopt from countries that are still dealing with considerable social problems and cultural change. This is either because the receiving country is aware of the difficulties the deprived children face and the extra parenting skills the adopters need, or because the countries in which the children were born have developed the services and cultural awareness to wish to keep their own citizens. Through counselling the patient(s) can assess whether or not they wish to pursue adoption as a course of action, and in particular address the change of focus from their own needs, biologi cal and emotional, to the needs of an existing child with no physical or genetic link to them. They can also be directed to information and services specific to the laws of the country in which they reside, and referred to specialist counselling in this field. Dreams and wishes could centre on a child who comes, for example, with the problems of low achievement or experiences of loss and low self-esteem. A child could be set up to fail and trauma and rejection can come about (Brebner, Sharp & Stone, 1985). If this happens there is the possibil ity of marital disharmony or a lack of bonding with one of the adoptive parents (Royal College of Obstetricians & Gynaecologists, 2000). In these instances the expectations of older children about such matters as the disruption to their lives need to be taken into account. It could also be that previous children believe they are not sufficient to meet their parents� needs and that they have failed their parents in some way. For many months or years they have been concentrating on their own needs and treatment and it is difficult to focus on the needs of a small child who will grow to adulthood with needs and wishes of their own (Triseliotis, 1973). This can lead to adopted children feeling angry or poorly adjusted in later life (Triseliotis, 1973). This means that the parents need to understand issues of difference, unintended or intended racism, as well as be prepared to help their child with identity problems that may arise (Thoburn, Norford, & Rashid, 2000). The number of children for adoption alone is not the only reason they may not achieve their goal. They will now face the possibility of being assessed on social and personal grounds and this can be even more distressing for some people than finding out they have a medical problem over which they have no control. In this particularly sensitive area of transfer from a medical to a social route to achieve parent hood it is particularly important that the decision to change a course of action is based on infor mation and education on what might lie ahead for the prospective parents. In such requests there is, in general, no fertility problem in the medical sense of the word. The treatment is justified more on social than on medical grounds since these requests are motivated not by the infertility of but by the absence of a male partner. The absence of the influence of a father figure and the homosexuality of the mother(s) are supposed to have a negative impact on the child�s development, especially where the psychosexual and social development is con cerned. Research concerning children raised in this type of family does not support these as sumptions (Brewaeys, 1997). The homosexual partners have a common wish to raise a child from birth in their family. In addition, the search for information about other possible solutions to resolve their �social� infertility can be laborious.
Genes generic meclizine 25 mg with visa symptoms vomiting diarrhea, through the proteins they encode cheap 25 mg meclizine mastercard medicine descriptions, determine how efficiently foods and chemicals are metabolized effective meclizine 25mg medicine bow, how effectively toxins are detoxified generic meclizine 25mg otc symptoms 8dp5dt, and how vigorously infections are targeted. Genetic diseases can be categorized into three major groups: single-gene, chromosomal, and multifactorial. A gene can mutate in many ways, resulting in an altered protein product that is unable to perform its normal function. Other mutations include the loss (deletion) or gain (duplication or insertion) of a single or multiple base(s). The altered protein product may still retain some normal function, but at a reduced capacity. In other cases, the protein may be totally disabled by the mutation or gain an entirely new, but damaging, function. The outcome of a particular mutation depends not only on how it alters a protein�s function, but also on how vital that particular protein is to survival. In addition to mutations in single genes, genetic diseases can be caused by larger mutations in chromosomes. Chromosomal abnormalities may result from either the total number of chromosomes differing from the usual amount or the physical structure of a chromosome differing from the usual structure. The most common type of chromosomal abnormality is Chapter 1: Genetics 101 7 Image Credit: U. Structural chromosomal abnormalities include deletions, duplications, insertions, inversions, or translocations of a chromosome segment. Although multifactorial diseases can recur in families, some mutations such as cancer can be acquired throughout an individual�s lifetime. Alterations in behavior or the environment such as diet, exercise, exposure to toxic agents, or medications can all influence genetic traits. Single-gene diseases are usually inherited in one of several patterns, depending on the location of the gene. Five basic modes of inheritance for single-gene diseases exist: autosomal dominant, autosomal recessive, X-linked dominant, X-linked recessive, and mitochondria. While mutations are generally associated with disease and are relatively rare, polymorphisms are more frequent and their clinical significance is not as straightforward. Although some genetic variations may cause or modify disease risk, other changes may result in no increased risk or a neutral presentation. Understanding the clinical significance of genetic variation is a complicated process because of our limited knowledge of which genes are involved in a disease or condition and the multiple gene-gene and gene-behavior-environment interactions likely to be involved in complex, chronic diseases. New technologies are enabling faster and more accurate detection of genetic variants in hundreds or thousands of genes in a single process. Selected References Department of Energy, Human Genome Project Education Resources This chapter provides information about the importance of clinical signs that may be suggestive of a genetic disease, family history, the different uses of genetic testing, and the different types of genetic diseases. Mutations may be inherited or developed in response to environmental stresses such as viruses or toxins. The ultimate goal of this manual is to use this information to treat, cure, or, if possible, prevent the development of disease. Clinical and laboratory testing, if appropriate and available Although primary care providers may not always be able to make a definitive diagnosis of a genetic disease, their role is critical in collecting a detailed family history, considering the possibility of a genetic disease in the differential diagnosis, ordering testing as indicated, and when available, appropriately referring patients to genetic specialists. The occurrence of the same condition such as multiple miscarriages, stillbirths, or childhood deaths in more than one family member (particularly first-degree relatives) is suggestive of a genetic disease. Other clinical symptoms suggestive of a genetic disease include developmental delay, mental retardation, and congenital abnormalities. Dysmorphologies (unusual physical features), as well as growth problems, can be suggestive of a genetic disorder. Although these clinical features may be caused by a number of factors, genetic conditions should be considered as part of the differential diagnosis, particularly if the patient expresses several clinical features together that might be indicative of a syndrome. Some physical features such as wide-set or droopy eyes, flat face, short fingers, and tall stature may appear unique or slightly different than the average. Even though these rare and seemingly mild features may not immediately be suggestive of a genetic disease to a primary care provider, an evaluation by a genetics specialist may be helpful in identifying the presence of a genetic disease. Genetic conditions should not be ruled out in adolescents or adults, though many genetic conditions appear during childhood. Genetic diseases can remain undetected for several years until an event such as puberty or pregnancy triggers the onset of symptoms or the accumulation of toxic metabolites results in disease later in life. Early detection of these diseases can lead to interventions to prevent the onset of symptoms or minimize disease severity. This type of testing is typically offered � Newborn Screening to individuals who have a family history of a genetic disorder or � Carrier Testing people in ethnic groups with an increased risk of specific genetic � Prenatal Diagnosis conditions. If both parents are tested, the test can provide � Diagnostic/Prognostic information about a couple�s chance of having a child with a specific � Predictive/Predispositional genetic condition. This type of testing is offered to couples with an increased risk of having a baby with a genetic or chromosomal disorder. A tissue sample for testing can be obtained through amniocentesis or chorionic villus sampling (see Appendix H). Predictive testing can identify mutations that increase a person�s risk of developing conditions with a genetic basis such as certain types of cancer.
As with administration of any drug related product buy meclizine 25mg with visa treatment 5th metatarsal fracture, there is the risk for reaction discount meclizine 25mg with visa crohns medications 6mp, including severe anaphylactic allergic reactions purchase meclizine 25 mg medicine world nashua nh. I am aware of this risk and do not hold responsible the person administering the drug buy meclizine 25mg cheap medicine 19th century, the pharmacy, or any other staff for any adverse reaction due to the administration of this vaccine/drug. Signature: Printed Name: (Parent or Guardian if Required) Date: Consent for follow-up injections: Date Medication Dose Number Administered Any change(s) to previous Patient of by information provided above Initials) Copyright � 2010, Dalhousie University Reproduction of this form is prohibited without written permission from Dalhousie University, Continuing Pharmacy Education. Copyright � 2010, Dalhousie University Reproduction of this form is prohibited without written permission from Dalhousie University, Continuing Pharmacy Education. Singh, Pablo Perel, Andrew Hutchings, Dario Camellino, 6 7 8 9 10 11 Sarah Mackie, Andy Abril, Artur Bachta, Peter Balint, Kevin Barraclough, Lina Bianconi, 12 13 14 15 5 Frank Buttgereit, Steven Carsons, Daniel Ching, Maria Cid, Marco Cimmino, 16 17 18 2 Andreas Diamantopoulos, William Docken, Christina Duftner, Billy Fashanu, 19 19 2 20 21 Kate Gilbert, Pamela Hildreth, Jane Hollywood, David Jayne, Manuella Lima, 22 23 24 25 Ajesh Maharaj, Christian Mallen, Victor Martinez-Taboada, Mehrdad Maz, 26 19 27 19 28 Steven Merry, Jean Miller, Shunsuke Mori, Lorna Neill, Elisabeth Nordborg, 19 19 6 29 18 Jennifer Nott, Hannah Padbury, Colin Pease, Carlo Salvarani, Michael Schirmer, 30 31 32 33 Wolfgang Schmidt, Robert Spiera, David Tronnier, Alexandre Wagner, 2 34 2 Madeline Whitlock, Eric L. Guidelines and recommendations are intended to promote beneficial or desirable outcomes but cannot guarantee any specific outcome. The American College of Rheumatology is an independent, professional, medical and scientific society which does not guarantee, warrant, or endorse any commercial product or service. Cid has received consulting fees, speaking fees, and/or hono Ernesto, Department of Rheumatology, Rio de Janeiro, Brazil; 22Ajesh raria from Centocor, Roche, and Bristol-Myers Squibb. Jayne has received consulting fees, tabria, Hospital Universitario Marques de Valdecilla, Facultad de speaking fees, and/or honoraria from Roche/Genentech, and research Medicina, Servicio de Reumatolog a, Santander, Spain; 25Mehrdad funding from the company. Mori has received research funding Kumamoto Saishunsou National Hospital, Department of Rheumatol from Bristol-Myers Squibb. Salvarani has received consulting fees, ogy, Clinical Research Center for Rheumatic Diseases, Kohshi, speaking fees, and/or honoraria from Novartis. Dasgupta has received consulting fees, speaking cine, Sao Paulo, Brazil;~ 34Eric L. Submitted for publication February 20, 2015; accepted in Mackie has received consulting fees, speaking fees, and/or honoraria revised form July 13, 2015. If uncertainty existed, a ists in general [internal] medicine and rheumatologists). The clinical evaluation should be directed toward exclusion of rele vant mimicking (eg, non-inflammatory, inflammatory (such as giant cell arteritis or rheumatoid arthritis), drug-induced, endocrine, infective and neo plastic) conditions. This will help to exclude mimicking conditions and establish a baseline for monitoring of therapy. Additional investigations such as chest radiographs may be considered at the discretion of the physician in order to exclude other diagnoses. A number of equally low to moderate quality studies, however, failed to demonstrate an association between these factors and relapse/prolonged therapy (27�30,32�44). Follow-up visits are suggested every 4�8 weeks in the first year, every 8�12 weeks in the second year, and as indicated in case of relapse or as prednisone is tapered and discontinued. It is important for patients to have rapid and direct access to advice from doctors, nurses or trained allied healthcare staff to report any changes in their condition such as flares and adverse events. A higher initial prednisone dose within this range may be considered in patients with a high risk of relapse and low risk of adverse events, whereas in patients with relevant comorbidities (eg, diabetes, osteoporosis, glaucoma, etc. The panel strongly recommends individualizing dose tapering schedules, predicated to regular monitoring of patient disease activity, laboratory markers and adverse events. Initial tapering: Taper dose to an oral dose of 10 mg/day prednisone equivalent within 4�8 weeks. Relapse therapy: Increase oral prednisone to the pre-relapse dose and decrease it gradually (within 4�8 weeks) to the dose at which the relapse occurred. Tapering once remission is achieved (following initial and relapse therapies): Taper daily oral prednisone by 1 mg every 4 weeks (or by 1. The algorithm assumes the consideration of overarching principles emphasizing the importance of assessing comorbidities, other relevant medications and possible risk factors for steroid-related side effects and relapse/ prolonged therapy. In addition, patients diagnosed in primary care should be considered for specialist referral, particularly in case of atypical presenta tion (such as peripheral inflammatory arthritis, systemic symptoms, low inflammatory markers, age,60 years), experience or high risk of therapy related side effects and/or relapse/prolonged therapy. A minimal clinical and laboratory dataset should be documented in each patient before prescribing therapy. A number of studies, how ever, failed to demonstrate association between these factors and relapse (48�51,54,67�78). Definitions of remission and relapse used in clinical studies are summarized in Dejaco et al (65). Relapse therapy: increase dose to the previously effective (ie, pre-relapse) dose. The panel did not construct case related to other conditions (eg, co-existing osteoarthritis). A more specific statement is not possible because of laboratory markers and adverse events. A higher initial in 4�8 weeks) to the dose at which the relapse prednisone dose within this range may be considered in occurred. Tapering once remission is achieved (following adverse events, whereas in patients with relevant comor initial and relapse therapies): Taper daily oral bidities (eg, diabetes, osteoporosis, glaucoma, etc. What is the optimal strategy for shared primary and specialty care including recommendations for specialist referral How can patients be better involved in treatment decisions, and are there any decision aids Patients may benefit from exercise by maintaining muscle mass and function as well as by fall prevention especially in the frail. Which targeted therapies could be developed based on new knowledge of disease mechanisms Bolded points indicate the top 5 items of the research agenda according to the opinion of the guideline panel. There was moderate to high quality of evidence (QoE) Future studies are necessary to clarify this issue.
We also ran a duration task (visual) generic meclizine 25 mg fast delivery medicine 0552, where we measured sensitivity for duration judgments and duration compression after speed adaptation purchase 25 mg meclizine overnight delivery symptoms stomach ulcer. Temporal sensitivity decreased with age regardless of the task meclizine 25mg lowest price symptoms 6dpiui, suggesting a widespread effect of aging on time perception generic meclizine 25mg without prescription medicine to help you sleep, most likely reflecting a general cognitive impairment. Temporal recalibration decayed with age for multisensory and sensorimotor, but not for unisensory stimuli. Most importantly, the effect of adaptation agreed with the Bayesian integration theory in the judgment of visual stimuli (unisensory temporal order, visual duration), whereas audiovisual and sensorimotor stimuli were recalibrated following a lag adaptation mechanism (Miyazaki, Yamamoto, Uchida & Kitazawa, 2006). Results from our study show that healthy aging selectively impairs the recalibration of temporal order between sensory modalities and between the sensory and the motor systems, and that a general loss in temporal sensitivity in elderly individuals might be related to an overall cognitive decline. During the visual-kinesthetic task, human subjects freely moved a computer mouse (or joystick, depending on the experiment) and reported which of the two cursors simultaneously visible on a high-speed computer monitor was driven by the mouse. Note that the since the mouse was self-driven, the underlying causal information arises solely from reafferent sources in this case. We systematically varied the temporal parameters of the cursors, including their spatial and temporal jitter. We found that when the variance of both cursors was relatively low (temporal jitter of < 4 Hz and/or spatial jitter of < 20 min arc on average), subjects performed well above chance levels (d� > 2, p < 0. However, with increasing cursor variance, subjects were increasingly likely to perceive the cursor with smaller variance as the one driven by the mouse. Indeed, sufficiently large cursor variance values could significantly override synchrony information (d� < -2, p < 0. Similar results were obtained during a similar visual-haptic task in which the visual object was synchronized with the haptic object in real time using an embedded rotation/position sensor (Hegde, 2016). Together, these results suggest that brain has an internal estimate of the reliability of its own reafferent information, and can override the inferred causal structure when it is inconsistent with other sensory information. Multisensory Integration Title: Temporal probabilistic inference in three sensory modalities 1 1 2 1,2 Authors: *M. Since fast ecologic cues happen on a short, continuous timescale, the brain has to model densely populated event horizons spanning intervals of several seconds. This temporal probabilistic inference requires estimation of elapsed time as well as event probability over time. In this work, we study how the brain models these stochastic sources of information in three different sensory modalities, namely vision, audition and somatosensation. Additionally it is not known if this process is similar across the different sensory modalities. We then demonstrate that there are significant differences between modalities, indicating peripheral processing, but also a prevalent common pattern across the three modalities, suggesting shared central processing of temporal probability estimation. Ongoing magnetoencephalography recordings aim to identify the neural correlates of these mechanisms manifested in behaviour. Physiological Properties of Neurons Support: Bard Summer Research Intitute Title: Midbrain neurons show temporal retuning of intrinsic properties in response to patterned uni and multisensory stimulation Authors: *S. For example, one can expect homeostatic plasticity to drive spiking thresholds up for neurons that receive stronger synaptic inputs. Similarly, it is conceivable that neurons involved in the temporal analysis of sensory stimuli could preferentially respond to either faster or slower patterns of synaptic activation. In this study, we use the dynamic clamp technique to explore changes in the intrinsic temporal tuning of midbrain sensory neurons in Xenopus tadpoles in response to sensory stimulation. We exposed animals to 3 hours of either visual, acoustic, or multisensory patterned stimulation that included light flashes, looming stimuli, and sound clicks. We then excited tectal neurons with simulated synaptic conductances of different temporal profiles in whole-cell patch-clamp mode, and measured their spike output. We asked whether, compared to controls, neurons in the tectum of tadpoles exposed to patterned stimulation retuned their temporal input-output functions, to potentially better adjust to this stimulation. We found that overall, the spiking in neurons from stimulated animals was homeostatically suppressed. When animals were exposed to looming stimuli, this suppression was weaker than for animals exposed to flashes, despite the fact that looming stimuli are known to induce stronger spiking in the tectum. Moreover, the temporal tuning of neurons in post-flash animals was strongly reshaped: while control and post-looming neurons spiked more in response to slower simulated synaptic conductances that mimicked looming stimuli, post-flash neurons preferred faster simulated inputs that mimicked full field flashes. This suggests that neurons became selective for the temporal stimuli to which they were exposed. We also checked whether acoustic stimulation alone, or a multisensory combination of visual and acoustic stimuli would change temporal tuning in tectal neurons. We found that although the tectum is typically thought of as a primarily visual area, repeated acoustic stimuli reduced tectal excitability, without reshaping temporal tuning. In multisensory experiments, unexpectedly, a combination of sound and visual flashes had a weaker effect on homeostatic suppression than visual flashes alone. The temporal tuning for multisensory stimuli also differed from unisensory, and depended on the delay between acoustic and visual stimuli during training. Finally, we report some of the cellular mechanisms behind these homeostatic changes. For example, the sense of speed should be estimated based not only on the optical flow but also on the engine-drive sound and vibration. In what manner do such visual and audio tactile information affect each other to generate the sense of speed In the present study, we investigated cross-modal effects using a virtual motorcycle system. In previous studies using basic psychophysical tasks, two opposite types of cross-modal effects have been reported, namely the averaging effect.
Antitussive Despite the methodological issues there is suf cient properties of inhaled bronchodilators on induced cough 25mg meclizine mastercard medications vs grapefruit. Effect of bron ferences make the cough challenge of likely value in chodilators on the cough response to order 25 mg meclizine free shipping medicine 123 inhaled citric acid epidemiology studies buy cheap meclizine 25mg on line symptoms 6dpo, some aspects of clinical manage in normal and asthmatic subjects discount 25 mg meclizine fast delivery medications heart disease. Sensitivity of the cough re ex in esis testing it is dif cult to imagine a strategy to unravel patients with chronic cough. Cap quire validation in large studies using more clinical saicin cough receptor sensitivity test in children. PhD thesis, Department of Thoracic Medi References cine, Royal Brompton National Heart and Lung Institute, University of London, December 1992. Assessing the substance P-induced cough in normal subjects during laryngeal cough re ex and the risk of developing pneumo upper respiratory tract infection. Am J Respir Crit Care Med 1995; 152: celecoxib on bronchial responsiveness and cough re ex 2068�75. Effect of ration of cough and re ex bronchoconstriction by inhaled nedocromil sodium on the airway response to inhaled cap local anaesthetics. Effect of clonidine on induced cough and bron hydroxytryptamine and 5-hydroxytryptophan on sensi choconstriction in guinea pigs and humans. Pharmacological regulation of comparison of the effect of inhaled diuretics on airway the cough re ex�from experimental models to antitus re exes in humans and guinea pigs. Investigation of the sensitivity of the cough tion of capsaicin induced airway re exes in humans: effect re ex in humans. The utility of arti cially induced dac on the abnormal cough re ex associated with dry cough as a clinical model for evaluating the antitussive cough. J Asthma 1999; 36 (3): cough sensitivity decreases with successful treatment of 265�70. This high prevalence raises the question as to when child the aetiology of cough can be broadly divided into hood cough should be considered �normal� or patho groups of primary pathophysiology, although there is logical. In childhood, cough may be �normal� [4] or a undoubtedly an overlap in the pathophysiology of symptom of any respiratory illness and rarely of a non some diseases (Table 7. The management of childhood that faces the physician is deciphering whether the cough [4,5] differs from that of adults [6]; and pae cough is �normal� or �expected�, non-speci c or speci c. The pattern of respi quency of each category will depend on the setting, and ratory illness in children can be clearly different from general practitioners would more likely encounter �ex that in adults. For example, viruses associated with pected/normal� cough whereas in a tertiary setting spe the common cold in adults can cause life-threatening ci c cough would dominate. These descriptions and the illness in children, such as bronchiolitis and croup; the common and/or controversial aetiologies of childhood natural history of asthma in children is dominated cough are brie y discussed below. A complete clinical by decreasing severity with age and, in some, complete review of each speci c aetiology is beyond the scope of resolution [7] whereas asthma acquired in adulthood this chapter and can be found in standard paediatric usually persists. Extrapolation of adult cough literature to children can be harmful, for example the Cough categories suggestion of fundoplication for gastro-oesophageal re ux as the sole symptom of cough without evidence �Normal� or �expected� cough of secondary aspiration [8] is inappropriate for chil dren. Indeed current evidence suggests that it is erro Diagnosing this category of cough requires the most neous to extrapolate the three commonest causes of skill and experience [4]. All cough is arguably represen cough in adults (cough-variant asthma, postnasal drip, tative of some process. Infectious Acute, subacute Viral infections, mycoplasma, chlamydia, pneumocystis, etc. Eosinophilic bronchitis Airway clearance 1 Aspiration (a) Primary: bulbar lesions, laryngopalatal discoordination, cerebral palsy, Moebius syndrome, vocal cord palsy (b) Secondary: gastro-oesophageal re ux (c) Anatomical: laryngeal cleft, tracheo-oesophageal stula, tonsil�adenoid hypertrophy 2 Airway lesions (a) Primary: laryngomalacia, bronchomalacia, tracheomalacia (b) Secondary: external compression (vascular slings, tumours, etc. Presence of: Haemoptysis Recurrent pneumonia Exertional dyspnoea �Normal� or Non Chronic sputum production �expected� cough specific Wheeze cough Stridor Immune de ciency Cardiac abnormality Swallowing dif culties Dyspnoea Specific Chest deformity cough Clubbing Ausculatory abnormality Poor growth Fig. Non-speci c cough overlaps with both speci c cough and �normal or expected cough�, whereas speci c cough is respiratory impairment are absent. In non-speci c cough, there (1�34 per 24h) can be found in �normal� children free of is no serious underlying condition and the child is a respiratory infection in the previous 4 weeks [11]. Brief overview of common causes In this study, children with recent viral infections were and controversies not excluded but were considered well by their parents. The manifestation of the infection de and have a higher cough frequency during the day than pends on various pathogens, �host or patient� factors the night [12]. The aeti reported use of medications for coughs and colds in the ology and necessity of further investigations is usually 2 weeks before assessment was 167 and 87 per 1000 for evident from the presence of these pointers (Table 7. How proximately 35% of 8145 preschool-aged children had many children in the community with persistent cough used �over the counter� medications for cough in the do indeed have asthma is unknown. Both studies objectively measured cough, and the presence of cough re ects the presence of a which is crucial, since cough as an outcome measure is lower respiratory tract infection. Neither recommended way in ammation has been demonstrated in children prolonged or high doses of asthma-type therapy when with colds, not only in the active phase but also in those managing these children [30,31]. Transient en diagnosis must be withdrawn and the medications hanced cough sensitivity has also been shown in chil stopped [4,5]. Cough and asthma in children Recurrence of cough on cessation and elimination of There is little doubt that children with asthma may cough upon commencement of inhaled corticosteroids present with cough and that wheeze may be absent is sometimes necessary for con dent diagnosis [4]. Isolated cough has been original studies describing cough as a manifestation of postulated as a marker of asthma, and improper asthma showed that the cough responded within a interpretation of cough as a symptom was previously week to medications used for asthma during that era thought to be a key factor in the underdiagnosis of (theophylline and hypnotics) [34,35]. However, more recently increasing numbers of argued that the currently available more potent anti children are misdiagnosed as having asthma on the in ammatory medications for asthma would reduce basis of cough alone [22�24], although there is also on the symptoms as ef caciously, if not more so. However, going concern that children with signi cant asthma following an acute exacerbation of asthma, cough was symptoms are still being missed and consequently present in 23% of children [36]. The importance of cough in the dren whether the cough is related to concurrent viral diagnosis of asthma and the frequency of cough respiratory infections, the cause of asthma exacer variant asthma is debatable [23]. Current epidemiolog bations in 80% of children [37], or a marker of non ical, in ammatory and cohort studies suggest that most resolution of asthma is unknown. Markers of cough cough in children is not asthma [23,26,27] and most severity are known to correlate poorly with clinical, in cough in children spontaneously resolves [26,28].
25 mg meclizine visa. Necrotizing Fasciitis - Flesh Eating Bacteria.